

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Approximately 400,000 deaths are attributed annually to cigarette smoking, which represent one-fifth of all deaths, and lung cancer and ischemic heart disease have been reported to be responsible for approximately half of smoking-attributable deaths in the U.S (1). In Korea, smoking cessation has also become an important social issue because lung cancer has been reported to be the most rapidly increasing cause of death (2). However, the smoking rate of Korean men remained higher as 69.9% until 2001, compared with 71.2% in 1985 (3).
Tobacco dependence (TD) is an important barrier to smoking cessation because it creates the feeling an urgent need to smoke to avoid the withdrawal symptoms associated with dependence (4). Smokers with TD try to stop smoking more often than nondependent smokers but remain more likely to do more trials to quit smoking (4).
The rate of dependence among ever-users of a drug indicates the risk of developing dependence once an individual has been exposed to the drug. However, the proportion of smokers who has TD remains controversial. The earliest study on TD revealed that more than 90% of smokers are dependent (5), but recent studies suggest a significant proportion of smokers may not be dependent (6). The findings of the National Comorbidity Survey (NCS) by Breslau et al. (7) found that the prevalence of dependence among those who had smoked daily for a month or more at one time was 49.5%, and that the prevalence of lifetime nicotine dependence was 24.1%, which means that about 50% of ever-smokers develop lifetime dependence. However, no previous study has been conducted to determine current or 12-month dependence among ever-smokers, as mentioned by Hughes et al. (6), which is a measure of the risk of developing dependence after one has been exposed to tobacco smoke (8).
Thus, it would be informative to determine whether rates of TD among ever-smokers vary or are stationary. This could be achieved by performing longitudinal comparisons of the rates of current TD among ever-smokers, and the prevalence of ever-smokers and current TD. If rates of current TD among ever-smokers are changeable, attempts should be made to identify the factors that reduce the rate of dependence. Alternatively, if rates are stationary, plans should be directed toward preventing initial exposure.
The purpose of this study was to examine whether changes in the rates of 12-month TD have occurred among ever-smokers, and to investigate the prevalence, correlates, and psychiatric comorbidity.
MATERIALS AND METHODS
Procedure and participants
The data were derived from the national study by Lee et al. in 1984 (9) and the Korean Epidemiologic Catchment Area (KECA) study by Cho et al. in 2001 (10). Lee et al. (9) conducted this study in collaboration with the Korean Population Health Research Center and the Seoul National University College of Medicine from January 4 to February 23 in 1984, and Cho et al. (10) conducted jointly by the Korean Ministry of Health and Welfare and the Seoul National University College of Medicine from June 1 to November 30, 2001. The Institutional Review Board of Seoul National University Hospital approved this study.
The subjects enrolled in both studies were selected using a stratified, multi-stage, cluster sample design, which was based on the population census of the community registry offices in 1980 and in 2000. All family members from selected households were included in 1984, whereas only one person per household, chosen at random, i.e., an adult family member with the earliest birth 'day' without considering the month or year. From an initially selected 6,200 persons in 1984 and 7,867 households in 2001, a total of 5,025 face-to-face interviews (response rate 81.0%) in 1984 and 6,275 interviews (response rate 79.8%) in 2001 completed the Composite International Diagnostic Interview (CIDI), including the tobacco usage section.
Diagnostic tools
The 1984 study was conducted using the Diagnostic Interview Schedule-III (DIS-III) (11), which is a fully structured interviewing tool that has been used in a previous Epidemiologic Catchment Area (ECA) Study (12). On the other hand, the 2001 study was conducted using CIDI 2.1 (13), which was also a fully structured tool and had been used in the NCS (14). The Korean version of CIDI was validated according to the WHO guidelines (15). To compare prevalence at two time points, we diagnosed TD using DSM-III criteria for 1984 and 2001.
Respondents who satisfied all criteria of TD were diagnosed as having TD (16). The criteria of TD included; continuous use of tobacco for at least one month (criterion A), and at least one of the followings: an unsuccessful serious attempt to stop or significantly reduce the amount of tobacco use on a permanent basis; attempts to stop smoking had led to the development of tobacco withdrawal; the continued use pf tobacco despite a serious physical disorder (e.g. respiratory or cardiovascular disease) known by the individual concerned to be exacerbated by tobacco use. The DSM-IV diagnostic criteria included not only three criteria of TD but also tolerance, larger amount and longer duration of consumption, and reduced activities. Therefore, three criteria were used for diagnosing TD from the data of 2001 survey. The 12-month TD was defined as the respondents experienced any symptom of dependence within 12 month prior to interview. The ever-smokers defined as the respondents have smoked daily for more than one month during their lifetime. The never-smokers were defined as the respondents who had no experience of smoking or who were insufficient to fulfill the criteria of ever-smokers.
Statistical analysis
Weighted values were calculated for respondents and used to adjust data, in order to approximate the national population in terms of age and gender in each catchment area, as defined by the Korean National Statistical Office's 2000 census. All statistical analyses were based on respondent weighted data.
We compared the prevalence of ever-smokers, 12-month TD, and 12-month TD among ever-smokers between the 2001 and the 1984 by genders with multivariate logistic regression analyses, adjusting for age, marital status, and residence. Odds ratios (OR) and 95% confidence intervals were presented. Multivariate logistic regression analyses were also conducted on selected variables including gender, age, and marital status. We then investigated comorbidity associated with TD with other psychiatric disorders, namely, alcohol dependence, alcohol abuse, major depressive disorder, anxiety disorders, psychotic disorders, and somatoform disorders. Multivariate logistic regression analyses were conducted for each psychiatric illness in order to compare never-smokers (n=3,286 in 1984 and n=3,859 in 2001), ever-smokers without 12-month TD (n=865 in 1984 and n=1,192 in 2001), and those with 12-month TD (n=874 in 1984 and n=1,223 in 2001). Data were analyzed using the Statistical Package for the Social Sciences (SPSS) 11.0 version.
RESULTS
Longitudinal comparisons of the prevalence of 12-month TD among ever-smokers
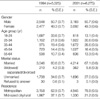
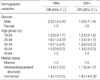
Sociodemographic data for the subjects were listed in Table 1, 2 presents the prevalence of ever-smokers, 12-month TD, and 12-month TD among ever-smokers. For men, the prevalence of ever-smokers significantly increased from 62.6% in 1984 to 71.9%, whereas the 12-month TD among ever-smokers showed no significant changes from 51.6% to 50.6%. For women, the prevalence of ever-smokers showed no significant changes from 5.7% to 6.1%, whereas the 12-month TD among ever-smokers significantly increased from 33.3% to 52.8%. As a result, the rates of 12-month TD among ever-smokers showed significantly higher in men in 1984 ( χ2=17.3, d.f.=1, p<0.001), but showed no significant gender difference in 2001 ( χ2=0.37, d.f.=1, p=0.54).
Comparisons between subjects with 12-month TD and ever-smokers
The adjusted ORs of sociodemographic variables for 12-month TD among ever-smokers are presented in Table 3. The variables associated with 12-month TD differed in 1984 and 2001. In 1984, 'male gender' was most strongly associated with 12-month TD (OR=2.3, 95% C.I.=1.5-3.4), but 'unmarried' was not associated (OR=1.4, 95% C.I=1.0-2.0). On the contrary, in 2004, 'unmarried' was associated with 12-month TD with a significance (OR=1.8, 95% C.I.=1.4-2.3), but the 'male gender' was not (OR=1.0, 95% C.I.=0.7-1.4).
Table 4 presents the adjusted ORs of lifetime psychiatric disorders. 'Alcohol dependence' was the only psychiatric disorder found to be associated with 12-month TD in 1984 and 2001. Compared with the ever-smoker group, the 12-month TD group was more associated with alcohol dependence and abuse, major depressive disorder, and anxiety disorder in 1984 but was only more associated with alcohol dependence in 2001 (OR=1.5, 95% C.I.=1.2-1.8). Compared with the never-smoker group, the ever-smoker group was more associated with alcohol dependence and abuse both in 1984 and 2001.
DISCUSSION
This is the first study to examine the prevalence of 12-month TD among ever-smokers in the general population. We also compared the prevalence in 1984 and 2001 in order to evaluate changes over the 17-yr period. Two major findings emerged from this study. First, 12-month TD was found in about 50% of ever-smokers, and gender differences between the rates of 12-month TD that was observed in 1984 disappeared in 2001. Second, subjects with 12-month TD showed a higher comorbidity with alcohol dependence.
Between 1984 and 2001, the prevalence of ever-smokers significantly increased in South Korea from 62.6% to 71.9% in men. However, the rates of 12-month TD to ever-smokers remained consistent at 50%. Previous studies showed that the prevalence of ever-smokers who had smoked daily for more than one month at some time was estimated as 49.5% by the NCS (7), and as 39.1% in young adults living in Detroit (17). On the other hand, the lifetime prevalence of TD was estimated to be 24.1% in the NCS (7), and 20.0% in the young adults in Detroit (17); nearly 50% of those who had ever smoked daily for a month or more. Although the prevalence of those with 12-month TD and ever-smokers were different in these studies, rates between the two were similar for these three previous studies and for the present study.
Dependence rates among drug ever-users indicate the risk of developing dependence after drug exposure (8). The results of this study indicate that tobacco use is associated with strong dependence. Anthony et al. (8) investigated drug dependence rates among ever-users by age group, and reported than tobacco showed the highest level of dependency, which was found in a study that included alcohol, cannabis, cocaine, stimulants, anxiolytics, analgesics, psychedelics, heroin, and inhalants; the dependence rate ranged from 3.7% for inhalants to 23.1% for heroin.
Gender differences between the rates of 12-month TD among ever-smokers that were observed in 1984 disappeared in 2001. The rate of 12-month TD among of female ever-smokers was about 50% in 2001, which was similar to those of male ever-smokers both in 1984 and 2001. A previous study conducted in the young adults in Detroit showed that the rate of TD among ever-smokers was about 50% and no gender difference was found in TD (17). The result implies that the susceptibility for TD is currently equal to both genders in Korea as in Western countries.
Moreover, TD was found to be closely associated with alcohol dependence, which concurs with previous studies (18-20). Some evidence indicates shared genetic influences concerning the development of tobacco and alcohol dependence (21), and of shared physiological effects, cross-tolerances, or cueing (22, 23). With regard to physiological effects, alcohol users may smoke to decrease some of the negative effects from alcohol (18). Alcohol dependence is another major health problem in Korea, with a report that the lifetime prevalence was estimated as 8.8% (24).
Significant associations have been found between TD and alcohol use disorders and mood and anxiety disorders (17-19, 25). Mood disorders are commonly found among Korean adults (26). It is noticeable in this study that TD was also significantly associated with other psychiatric disorders including alcohol abuse, major depressive disorder, and anxiety disorders in 1984 but not in 2001. This is mainly attributable to the exclusion criteria of the DSM-IV, where symptoms are not due to the direct physiological effects of a substance (27). We consider that it may be difficult to decide whether depression or anxiety results from tobacco use because subjects are more likely to agree that symptoms stem from TD rather than a psychiatric illness.
Although the results of the present study showed that the rates of TD among ever-smokers are consistent, our study had some important limitations. The first concerns the retrospective nature of the data used, as recall bias might have affected the accuracies of prevalence and illness duration data. Second, non-response might also have impacted the results, as it has been reported that non-respondents have higher rates of mental disorders than respondents. Third, TD was diagnosed with structured interviews by trained interviewers, not with clinical interviews by psychiatrists. There also are limitations on the diagnostic accuracy of TD. Lastly, cohort effects might have influenced the results. Although age and gender rates were similar between the 1984 and 2001 survey, they were different cohorts.
In conclusion, 12-month TD was found to be consistently experienced by 50% of ever-smokers, and those with dependence showed higher comorbidity with alcohol dependence. TD is a clear barrier to smoking cessation, and continued smoking increases mortality and morbidity. Further research is needed to diagnose vulnerable groups before exposure to tobacco in order to elucidate the mechanisms of TD and to allow adequate prevention planning.


 XML Download
XML Download