

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary pituitary carcinomas are very rare neoplasms defined as adenohypophyseal tumors with cerebrospinal and/or systemic metastasis. They represent approximately 0.2% of all operated adenohypophyseal neoplasms (1). The disease was first reported in 1931 by Cairns et al. (2) in a 25-yr-old woman with pituitary adenoma and intradural spinal cord metastasis. There have been more than 100 cases of pituitary carcinoma reported, including functional and nonfunctional tumors (3), but none in the Korean literature to the best of our knowledge. The histologic features of pituitary carcinomas are vary from typical adenoma to tumor with marked pleomorphism and frequent mitoses (4, 5). Here we report a case of pituitary carcinoma with left mandibular metastasis in a 36-yr-old woman.
CASE REPORT
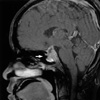
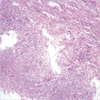
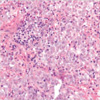
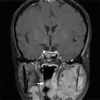
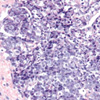
A 36-yr-old woman with a 3-week history of headache was presented at the outpatient otorhinolaryngology clinic for the evaluation of suspicious sinusitis in November 2005. Symptoms including nausea, vomiting, myalgia, and general weakness worsened despite ongoing antibiotic therapy. No lesion was found in the initial brain computed tomography (CT) scan. Twenty days later she reported right-side ptosis and amenorrhea. Magnetic resonance imaging revealed a 2.5-cm sellar and suprasellar mass with heterogeneous enhancement, and suspicious invasion to both cavernous sinuses and the left maxillary sinusitis (Fig. 1). The mass compressed the optic chiasm. Her serum prolactin level was 123.17 ng/mL before surgery. She underwent gross-total resection based on the initial diagnosis of pituitary macroadenoma with 3rd and 6th nerve palsy. Histologically, the resected tumor was composed of variable-sized nests and single cells mixed with adenohypophyseal cells, which appeared normal (Fig. 2). The tumor cells had polygonal vesicular nuclei with marked pleomorphism and prominent nucleoli. The cytoplasm was acidophilic and granular (Fig. 3). When presented, mitoses counted 3 per 10 high power fields (HPFs). Immunohistochemistry staining was strongly positive for prolactin (PRL) (Fig. 4), but negative for adenocorticotropic hormone (ACTH) and growth hormone (GH). Immunostaining was also positive for synaptophysin and p53 (Fig. 5A), but not for cytokeratin, vimentin or glial fibrillary acidic protein (GFAP). The Ki-67 labeling index (Fig. 5B) was high. Postoperative CT scanning revealed a residual nodular enhancement at the superior portion of the resected mass. Radiotherapy (total dose 5,040 Gy) was undertaken after surgery, based on the atypical morphology of the pituitary tumor and the presence of the residual enhanced mass. The prolactin level fell to 5.17 ng/mL after surgery and adjuvant radiotherapy.
The patient was readmitted 6 months later with a one-month history of left cheek and periauricular pain. The patient had problems opening her mouth, and painful swelling and local heating. Radiologic assessment revealed a soft tissue mass with cortical destruction and a permeative osteolytic lesion at the left mandibular ramus (Fig. 6). A partial mandibulectomy was performed. Grossly, the mandible and perimandibular soft tissue were involved by the tumor. The histologic features (Fig. 7) and the immunohistochemical results were identical to those observed in the previous pituitary tumor. Primary pituitary carcinoma was confirmed from the histopathologic findings and a metastasis. She died in August 2006, approximately 9 months after the initial diagnosis.
DISCUSSION
Pituitary carcinomas are rare adenohypophyseal neoplasms and their definition, diagnosis, therapy, and prognosis are controversial. Unlike other malignant neoplasms, the diagnosis of pituitary carcinoma is based on metastasis and not on histologic features such as invasion, cellular pleomorphism, nuclear abnormalities, mitotic activity, and necrosis. More than 100 cases of pituitary carcinoma have been reported worldwide (3), but this is the first report in Korea.
In a review of the literature on pituitary carcinoma, Pernicone et al. (1) reported the endocrinological subtypes include PRL-producing tumors (30%), ACTH-producing tumors (28%), GH-producing tumors (10%), thyroid-stimulating hormone-producing tumors (2%), gonodotropin-producing tumors (2%), and nonfunctioning tumors (26%). Malignant prolactinomas, such as the case described here, were the most common (26 cases) subtype of pituitary carcinomas reported (6). They predominantly occur in males (M:F=17:9), in middle age (range: 14-70 yr, mean: 43.6 yr), and have a poor prognosis. Most of the locations of metastasis are extra/intracranial and spinal sites (50%), but can involve other sites including bones and soft tissues (occiput, ribs, vertebra, sacroiliac joint, femur, and mandible), and parenchymal organs (lung, lymph node, liver, ovary, endometrium, and adrenal gland). In addition, nearly all pituitary carcinomas are identified as functioning, mitotically active, and invasive macroadenomas with a tendency for multiple metastasis.
Although the primary pituitary carcinomas have various histologic features, from monotonous proliferation of cells with uniform nuclei to cellular pleomorphism and prominent nucleoli, the cytologic atypia does not predict the tumor behavior. However, there is a slight trend towards a higher degree of cytologic atypia and increased mitotic activity in metastasis lesions compared with primary tumors (1). Our case had atypical morphology with frequent mitoses in both primary and metastasis tumors. The Ki-67 index was high in the primary and metastasis tumors (10% and 30%, respectively). In the study by Thapar et al. (7), the relationship between proliferative activity in pituitary adenomas and their invasiveness was investigated using the MIB-1 monoclonal antibody, which detects the Ki67 cell cyclespecific nuclear antigen. The growth fractions of noninvasive adenoma, invasive adenoma, and primary pituitary carcinomas were 1.37±0.15%, 4.66±0.47%, and 11.91±3.41%, respectively. In comparison with the above study, the Ki-67 labeling index in the primary and metastasis lesions of the present case exceeded the level reported for pituitary carcinomas. In addition, the p53 immunostaining reported for the tumor suppressor gene was 0%, 15.2%, and 100% for the noninvasive adenoma, invasive adenoma, and carcinoma, respectively (7). Our case was p53-positive in both the primary and metastasis pituitary carcinoma.
Histological changes in pituitary carcinoma after radiation therapy were reported by Yamashita et al. (8). After irradiation approximately three-fifths of tumor cells were unaltered and two-fifths showed degeneration. It was suggested the tumor necrosis after irradiation was not an apoptotic process but an irradiation effect because TUNEL staining of the nuclei of postirradiated cells was negative. However, nonirradiated pituitary carcinoma can show extensive necrosis (up to 50%), as in this case, whether or not apoptosis is involved.
The prognosis of pituitary carcinoma is known to be poor because of the extent of tumor dissemination at the time of diagnosis, with the mean survival time reported to be 2 yr (range 0.25-8 yr) (1). For malignant prolactinomas the latent period between initial diagnosis and detection of metastases ranged from 2 to 228 months, and most patients (80%) died within 18 months of metastasis development. In our case, the latent period was 6 months, and the patient died 3 months after metastasis developed.
In conclusion, pituitary carcinoma is a rare tumor involving cranio-spinal or systemic metastasis. Irrespective of the histological morphology, the behavior of primary pituitary neoplasms cannot be predicted. In view of the poor prognosis, atypical morphology including local invasion, increased mitosis, and a high proliferation index (as in this case), close follow-up is required for proper management.


 XML Download
XML Download