

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although gangliogliomas of the central nervous system are rather uncommon tumors that consist of a mixture of neoplastic glial cells and differentiated ganglion cells, the disease entity is well recognized. They occur most frequently in children and in adults younger than 30 yr old (1). Gangliogliomas are typically associated with a long history of intractable seizures because they most often arise in the temporal lobe; the prognosis is usually favorable (1). In contrast, anaplastic gangliogliomas are very rare and their clinical course is poorly understood (2-6). The anaplastic change in gangliogliomas is more frequent in the pediatric population (3, 6). Here, we report a case of anaplastic ganglioglioma identified histologically at initial resection in a middle-aged woman.
CASE REPORT
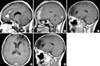
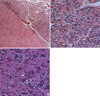
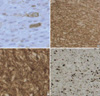
A 45-yr-old female patient presented with a history of headache and dizziness, both of which progressed slowly. A neurological examination showed nothing remarkable. Preoperative magnetic resonance imaging (MRI) revealed a left frontal lesion that was slightly hypointense on T1-weighted images and hyperintense on T2-weighted images. The lesion extended to the cingulate gyrus with peritumoral edema and strong contrast enhancement (Fig. 1A). Gross total resection of the tumor revealed a dark-brown, friable mass, consisting of a soft, aspiratable portion and a fibrous hypervascular nonaspiratable portion. Microscopically, the ganglioglioma contained atypical glial cells and scattered ganglion cells. The tumor cells infiltrated the gray matter and subarachnoid space (Fig. 2A). The tumor cells in the gray matter consisted of neoplastic ganglion cells and glial cells. Those in the subarachnoid space were mainly glial cells and showed increased cellularity, nuclear atypism, and occasional mitosis (Fig. 2B). The abnormally clustered ganglion cells lacked orderly distribution and polarity, and most had large nuclei with prominent nucleoli (Fig. 2C). The neoplastic ganglion cells were immunoreactive to synaptophysin and neuron specific enolase (NSE) (Fig. 3A, B). The atypical glial components were positive for glial fibrillary acidic protein (GFAP) (Fig. 3C). A diagnosis of anaplastic ganglioglioma was made. The patient recovered postoperatively without any neurologic deficits. MRI taken 12 days postoperatively showed multiple irregularly shaped enhancing lesions along the resection margin of the left frontal lobe and cingulate gyrus (Fig. 1B). Two weeks after surgery, she received one cycle of intravenous nimustine HCl (ACNU, 60 mg) and cisplatin (CDDP, 60 mg). Subsequently, radiation therapy was administered in 30 doses for a total dose of 6,000 cGy over five weeks, and additional three cycles of chemotherapy with the same regimen were given. During chemotherapy, she was managed for pancytopenia. Five months later, follow-up MRI revealed that the remaining mass in the cingulate gyrus and resection margin had disappeared (Fig. 1C). She has shown intact neurological status and no other complications until now, and the last follow-up MRI at 35 months postoperatively demonstrated no evidence of recurrence (Fig. 1D, E).
DISCUSSION
The incidence of gangliogliomas has been reported to range from 0.4% to 7.6% in a series of brain tumors in a pediatric population (7). Central nervous system gangliogliomas are usually benign. Although malignant variants of ganglioglioma are said to be rare, Russell and Rubinstein estimated the rate of malignant change to be approximately 10% (1). Considering other reports, anaplastic gangliogliomas seem to account for 3-5% of gangliogliomas (6). However, the incidence remains unknown. Although malignant variants commonly occur in the supratentorial regions, some occur in other regions (8-12). Recently, Blumcke and Wiestler (13) reported that these tumors tend to occur in older patients with a mean age of 35±14.5 yr (range 10-88 yr). Macroscopically, gangliogliomas are usually firm well-circumscribed masses with a granular appearance on cut sections (1). According to Russell and Rubinstein (1), the microscopic criteria for the diagnosis of ganglioglioma are as follows: the tumor consists of a mixture of glial cells and neurons; the glial cells consist mostly of astrocytes; and the cells are identified as neurons only if Nissl substance can be demonstrated by cresyl violet staining or if they give rise to neuronal processes, as demonstrated using modified Bielschowski or Bodian stains. For neurons to be considered neoplastic, they must be either clearly heterotopic (located away from the gray matter), or atypical (showing disorientation, bizarre shapes or sizes, and nuclei with hyperchromatism and frequent binucleation) (7). Confirmation of the neuronal component may require the use of immunohistochemical markers, including synaptophysin, neurofilament protein, NSE (1, 7), and NeuN. The astroglial components are positive for GFAP and S-100 proteins. In our case, we found neoplastic glial cells and neuronal cells that were clustered and lacked orderly distribution and polarity; most had large nuclei with prominent nucleoli. The tumor cells revealed definite immunoreactivity for synaptophysin, NSE, and GFAP. The Ki-67 labeling index (LI) in our case was 20%, while the reported Ki-67 LI in ganglioglioma is generally less than 10% (Fig. 3D) (6). Therefore, we made a diagnosis of diagnosed anaplastic ganglioglioma in our case.
The manifestation of malignant biological features in some gangliogliomas, as with other glial tumors, results from anaplastic histological features at initial resection (3, 9, 12, 14-19) (Table 1) or anaplastic transformation of a previously benign ganglioglioma (4, 8, 10, 11, 20-22) (Table 2). These tumors tend to occur in older patients compared with the usual onset age of ganglioglioma, especially anaplastic gangliogliomas found at initial resection.
Total removal is recommended and regarded as a good prognostic factor for the treatment of ganglioglioma without anaplastic features (2, 5, 7). The benefits of radiation therapy or chemotherapy for the treatment of ganglioglioma have not been clearly defined (4, 7). Although radiation therapy has uncertain benefits, it is generally given to patients with incomplete resection of the tumor or recurrent tumor, and to those with a tumor histology showing anaplastic features or oligodendroglial-like cells (7). Although the optimum treatment for anaplastic ganglioglioma has not been established, our patient, who was treated surgically with adjuvant therapy, is still alive without tumor progression or recurrence. This suggests that adjuvant radiation and chemotherapy is of some value.
The biological nature of these anaplastic variants is poorly understood because there are few documented cases. The survival rate is lower when the tumor is localized in the midline structures or when there are anaplastic features (2, 7, 23). Based on their multivariate analysis, Park et al. (24) reported that the two most important favorable prognostic factors affecting the overall survival were low tumor grade and gross total resection. However, other authors reported that the histological grade of the ganglioglioma is not a predictor of poor outcome (5, 7). Therefore, the prognosis of gangliogliomas with malignant histological features remains uncertain. Although predicting the prognosis of anaplastic gangliogliomas is difficult, some authors stated that cell kinetic studies, such as MIB-1 staining, may be useful for predicting the prognosis (6, 8).
Here, we report on a very rare case of anaplastic ganglioglioma that occurred in a middle-aged woman. Although the relationship between the clinical outcome and histological grade remains unclear and the effects of radiation therapy and chemotherapy on gangliogliomas are uncertain, adjuvant radiation therapy and chemotherapy appear to have been effective, at least so far. Further long-term studies on a larger number of ganglioglioma patients are necessary to better understand the clinical outcome and appropriate treatment strategies.


 XML Download
XML Download