

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prolonged pregnancy occurs in approximately 10% of all singleton pregnancies and is associated with an increased risk of fetal macrosomia, intrapartum fetal heart abnormalities, meconium staining, perinatal death, and cesarean delivery (1-3). An early prediction of this condition is important because several methods to decrease the rate of prolonged pregnancy, such as membrane stripping and outpatient prostaglandin therapy, have been already proposed (4, 5). Therefore there has been considerable interest in the development of tests for the prediction of prolonged pregnancy. These tests include fetal fibronectin, cytokine, or nitric oxide concentrations in cervicovaginal secretions and cervical length as determined by ultrasonography (6-10).
Cervical length measured by transvaginal ultrasound in the second trimester has been well known to be effective in identifying pregnancies at high-risk of spontaneous preterm delivery (11-16). Recent studies have reported that sonographic measurement of cervical length at term is a useful predictor of the likelihood of successful induction of labor and the spontaneous onset of labor in a 7-day period (17-21). Moreover, Romero et al. have proposed that cervical ripening is part of the common terminal pathway of human parturition, which includes uterine contractility and membranedecidua activation (22). These observations suggest that a passively shortened or dilated cervix may play a role in the mechanisms responsible for the initiation of parturition (preterm and term). Therefore if the shorter the cervix, the greater the risk of preterm delivery, the likelihood of successful induction of labor and the spontaneous onset of labor, it is possible that a longer cervix may predict a higher risk of prolonged pregnancy. The purpose of this study was to determine whether the transvaginal ultrasonographic measurement of cervical length at 20 to 24 weeks and 37 weeks can predict prolonged pregnancy in nulliparous women.
MATERIALS AND METHODS
Study design
This was a prospective observational study conducted at Seoul National University Bundang Hospital (Seongnam, Korea) between June 2004 and May 2006. Women attending the antenatal clinic were enrolled at 37 weeks. In our institution ultrasound examination is carried out routinely at 11-14 weeks and at 20-24 weeks of gestation. The scan at 20-24 weeks included fetal examination and the option of having a transvaginal scan to measure cervical length as a screening test for spontaneous preterm delivery. The inclusion criteria were: 1) nulliparous women; 2) singleton pregnancy; 3) live fetus with vertex presentation; 4) intact amniotic membranes; 5) known gestational age confirmed by ultrasound measurement of crown-rump length (CRL) (gestational age was corrected on the basis of CRL measurement if a discrepancy of 7 days or more exists); 6) with sonographically measured cervical length between 20 and 24 weeks; 7) no pregnancy complications (i.e., fetal growth restriction, preeclampsia, and major fetal abnormalities); 8) absence of labor; 9) no history of previous uterine surgery. Prolonged pregnancy was defined as a pregnancy that extended beyond 41 weeks and 2 days (289 days) (this definition was developed because we usually induced labor in patients who did not go into spontaneous onset of labor by that date). Week of gestation was defined as completed week; i.e., week 37 refers to 37.0 weeks to 37.6 weeks menstrual age. The results of the ultrasound were blinded for the clinicians. This study was approved by the institutional review board of our institution Seoul National University Bundang Hospital. Informed consent was obtained prior to enrollment in the study.
Transvaginal ultrasound of the cervix
Transvaginal ultrasonographic assessment of the cervical length was performed by one of the authors at 20-24 weeks using an Aloka SSD 5500 (Aloka Co. Ltd, Tokyo, Japan) ultrasound machine with a 6.0 MHz transducer and at 37 weeks using an Envisor (Philips Medical System, Netherlands) ultrasound machine with a 6.0 MHz transducer. Women were asked to empty their bladder and were placed in the dorsal lithotomy position. The probe was gently placed at the anterior fornix of the vagina to obtain a sagittal view of the complete cervix, including the internal os, external os, and endocervical canal. The probe was slowly withdrawn until the image blurred and then the insertion pressure was increased only enough to restore a clear cervical image. This cervical image was magnified to at least 75% of the screen and the electronic markers were placed at the furthest points between the internal os and external os, then cervical length was measured as a straight line. The shortest of three measurement obtained was taken as the cervical length.
Statistical analysis
Univariate analysis was conducted using the Mann-Whitney U test or the χ2 test. Receiver operating characteristic (ROC) curves were constructed to describe the relationship between the sensitivity (true-positive rate) and the false-positive rate for the cervical length in predicting prolonged pregnancy. Pearson correlation analysis was used to determine the relationship between sonographically measured cervical length and gestational age at delivery. p values of <0.05 were considered statistically significant.
RESULTS
During the study period, 184 consecutive women met the inclusion criteria in this study. Of these, 35 women had labor induced before 41 weeks and 2 days because of oligohydramnios (n=28), non-reassuring non-stress test (n=3), and request for social reason (n=4). Thus, these women were excluded from the study, leaving a total of 149 women qualified for inclusion. Spontaneous onset of labor and delivery at or before 41 weeks and 2 days occurred in 126 (85%) women. In 23 women (15%) that remained undelivered beyond 41 weeks and 2 days, 20 had induction of labor and 3 had spontaneous onset of labor. Cervical length was successfully measured in all cases and the mean (±standard deviation) cervical lengths at 20 to 24 weeks and 37 weeks were 39±6 mm and 28±6 mm, respectively.
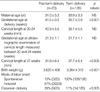
Table 1 presents the clinical characteristics and obstetric outcomes of patients according to the study group. No significant differences were found in terms of median maternal age and median gestational age at ultrasound examination of cervical length measured between 20 and 24 weeks between the study groups. However, women going beyond term had a significantly higher rate of cesarean delivery and greater mean birth weight than did those with spontaneous term delivery. Moreover, the median cervical length at 37 weeks was significantly longer in women going beyond term than in those with spontaneous term delivery, but the median cervical length at 20-24 weeks were not significantly different between the two study groups.
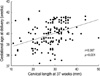
Fig. 1 displays the ROC curve for sonographically measured cervical length at 37 weeks in predicting prolonged pregnancy. The curve constructed for sonographically measured cervical length was above the 45° line, indicating that there was a significant relationship between this variable and prolonged pregnancy (area under the curve 0.702; SE 0.060; p<0.005). The best cut-off value for the prediction of prolonged pregnancy was 30 mm with a sensitivity of 78% and a specificity of 62%. A significant positive correlation between sonographically measured cervical length at 37 weeks and gestational age at delivery was noted (r=0.387, p<0.0001) (Fig. 2). However, there was no correlation between cervical length at 20-24 weeks and gestational age at delivery.
DISCUSSION
The results of our study clearly demonstrate that cervical length assessed by transvaginal ultrasonography at 37 weeks can predict the likelihood of prolonged pregnancy and is associated with the gestation at spontaneous onset of labor in low-risk nulliparous women. Furthermore, our data indicate that these associations did not exist as early as 20 to 24 weeks. Similar observations have been made in other gestational ages (i.e., at 11 to 14 weeks and 22 to 24 weeks of gestation) in the setting of spontaneous preterm delivery (12, 13).
Several investigators have reported that measurement of cervical length in the second trimester provides accurate prediction of risk for spontaneous preterm delivery and this risk is inversely correlated with cervical length (11-16). However, there are few reports on cervical length in the second trimester of pregnancy in relation to prolonged pregnancy. Some studies have begun cervical assessment at 37 weeks and demonstrated that cervical length at 37 weeks is associated with the incidence of prolonged pregnancy and the spontaneous onset of labor in a 7-day period (9, 10, 21). To our knowledge, this is the first report to examine the relationship between cervical length in the second trimester and the occurrence of prolonged pregnancy. The results are unexpected, in that relationship found in spontaneous preterm delivery does not exit (i.e., the longer the cervical length in the second trimester, the higher the rate of prolonged delivery). These findings imply that cervical assessment provide sensitive prediction of spontaneous delivery (preterm or term) within the next some weeks, not the next some months, regardless of whether this assessment is performed in the second trimester or at term.
A major finding in this study is that cervical length at 37 weeks can predict the likelihood of prolonged pregnancy. This finding is in keeping with the observation made by Ramanathan et al. who demonstrated that measurement of cervical length at 37 weeks can be used to determine the likelihood of prolonged pregnancy and the risk of cesarean section in those requiring induction for prolonged pregnancy (9). Conflicting finding, however, has been reported by Vimercati et al. (10). They demonstrated that the measurement of cervical length at 39 weeks and 40 weeks was significantly shorter in a group who had spontaneous onset of labor before 41 completed weeks of gestation than in that who did not, but the measurement of cervical length was similar in both group at 37 weeks and 38 weeks. The disparity among these studies is probably attributable to a combination of factors, including the definition of prolonged pregnancy, the study population to participate (i.e., nulliparity or primiparity), and sample size. Nulliparity was chosen as the enrollment criterion of our study because primiparity and prior prolonged pregnancy are the most common identifiable risk factor for prolongation of pregnancy (9, 23, 24).
It is noteworthy that a significant positive correlation between cervical length at 37 weeks and gestational age at delivery was noted. This finding is consistent with the observations of Ramanathan et al. who documented a high association between cervical length at 37 weeks and gestation at spontaneous onset of labor (9). Moreover, in the current study, cervical length at 37 weeks ≥30 mm had a sensitivity of 78% and a specificity of 62% in the prediction of prolonged pregnancy. These data have several clinical implications for the management of patients at term. First, if routine measurement of cervical length at 37 weeks can identify patients at high risk of prolonged pregnancy, the incidence of prolonged pregnancy or the risks associated with prolonged pregnancy will be reduced because simple method to promote spontaneous onset of labor (i.e., membranes stripping and outpatient prostaglandin therapy) was already proposed (4, 5). Second, these data may be utilized in individualizing the timing of elective cesarean section rather than performance of this operation at 38 weeks. Third, from the patients' point of view these data may give patients information to arrange their social activities and to deal with their anxiety.
Our study has demonstrated that the mean cervical lengths at 20 to 24 weeks and 37 weeks are, respectively, 39 mm and 28 mm in singleton low-risk pregnancies delivered at or beyond term. These findings are similar to those of previous reports (9, 12, 25). Moreover, our data indicated that the cervical length decreased from the second trimester to term and this spontaneous shortening was, however, more pronounced in women delivered at term than in those going beyond term. The mean cervical length in women delivered at term decreased from 39.1 mm to 27.7 mm. On the other hand, in women going beyond term, the shortening of the cervix was from 40.9 mm to 31.9 mm between the 20-24-week and the 37-week evaluations. These findings indicate that the relatively slow rate of spontaneous cervical shortening between the second trimester and term pregnancy might be related to the occurrence of prolonged pregnancy. In a similar study, Vimercati et al. also reported that women who remained undelivered beyond 41 weeks has a delayed effacement process and the measurement of cervical length at 41 weeks in these women would possibly show the same pattern as that at 39 weeks in women who had spontaneous onset of labor before 41 weeks (10). On the other hand, in the context of spontaneous preterm delivery, Carvalho et al. have found that there is a spontaneous shortening in the pregnant cervix from the first to the second trimester of pregnancy and this shortening is more rapid in pregnant women who deliver prematurely (12).
A limitation of the current study is that cervical length was measured as a straight line because from the practical point of view, it is reasonable to measure the linear distance between the internal and external os. Although in cases with a curved cervix the longer the measurement taken along the endocervical canal, the longer inevitably the measurement of cervical length taken as a straight line, cervical length in our study population, especially measured at 20-24 weeks, may not represent true cervical length.
In conclusion, cervical length at 37 weeks can predict the likelihood of prolonged pregnancy and is associated with the gestation at spontaneous onset of labor in low-risk nulliparous women. However, cervical length at 20 to 24 weeks is associated with neither prolonged delivery nor the gestation at spontaneous onset of labor.

 XML Download
XML Download