

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Mechanical ventilation is the main life-sustaining therapy for patients with acute respiratory distress syndrome (ARDS). However, if not carefully performed, it may precipitate or aggravate lung injury (1). Two main mechanisms causing this ventilator-induced lung injury (VILI) are overdistension due to a large tidal volume, and repeated opening and closing of collapsed lung units during the respiratory cycle (1-3). Lung-protective strategy, which includes tidal volume restriction and optimization of positive end expiratory pressure (PEEP), has been proposed for patients with ARDS in order to minimize VILI (4-6). Such strategy tries to avoid high alveolar pressures by using small tidal volumes and attempt to keep alveoli open at end-expiration by use of sufficient PEEP (2, 4, 6). It is now accepted by most investigators that restricting tidal volume is beneficial for ARDS patients (6).
However, the best way to set PEEP in patients with acute lung injury (ALI) has been a subject of intense debate. The traditional approach to titrating PEEP has been to use the 'least' PEEP approach (6, 7). Investigators have studied other methods to titrate PEEP (8-11), but none has been shown to be superior to others. Recently, some investigators have advocated using the inflation limb of the pressure-volume (PV) curve to guide PEEP levels in early ALI (2). However, because PEEP is a force that opposes derecruitment rather than being the pressure that actually recruits the lungs, titration of PEEP may be better accomplished by PEEP decrements after initial recruitment of the collapsed lung (12, 13). We previously reported that PEEP titration by use of decremental PEEP after a recruitment maneuver (RM) was effective in improving oxygenation and was generally well-tolerated (14). However, whether this approach has any benefit compared to the PEEP titration method that is based on the inflation limb of the PV curve is not known (15, 16).
The objective of this study was to observe the sequential effects of two methods for setting PEEP that can be clinically applied; one based on the inflation limb and the other on the deflation limb of the PV curve after recruitment maneuver (RM) in a canine acute lung injury model.
MATERIALS AND METHODS
This study was reviewed and approved by the Animal Care and Use Committee of the Samsung Biomedical Research Institute, and was performed in accordance with the Institute for Laboratory Animal Resources guidelines for the care and use of laboratory animals.
Animal preparations and measurements
Six mongrel adult male dogs weighing between 17.4 and 21.6 kg were anesthetized with xylazine (5 mg/kg) and ketamine (35 mg/kg) and restrained in the supine position. A cuffed endotracheal tube (6.0 mm internal diameter) was placed in the trachea and secured in position. The animals were ventilated with a Servo 900C ventilator (Simens Elma AB, Solna, Sweden) in volume-controlled mode with a PEEP of zero (ZEEP), a tidal volume (VT) of 10 mL/kg, an inspiratory: expiratory time ratio of 1:2, a pause time of 10%, an inspired oxygen fraction (FiO2) of 1.0, and a respiratory rate of 20 breaths per minute. The respiratory rate was then set to achieve normocarbia and was maintained constantly until the end of the study. Mechanical ventilation was continued in the same manner throughout the experiment, except for the adjustments of PEEP levels described subsequently. Anesthesia and muscle paralysis were maintained by continuous infusion of sodium pentobarbital (5 mg/kg/hr) and vecuronium (0.125 mg/kg/hr) via an intravenous infusion pump, and normal saline (10 mL/kg/hr) was infused as a maintenance fluid.
The right femoral artery was catheterized for blood gas determinations (288 Blood Gas Analyzer, CIBA-Corning Diagnostic Corp., Medfield, MA, U.S.A.) and monitoring of arterial pressure. A Swan-Ganz catheter (5 Fr, Baxter Healthcare Corp., Irvine, CA, U.S.A.) was inserted through the right external jugular vein for measuring cardiopulmonary hemodynamics and for sampling mixed venous blood. Heart rate, electrocardiogram, mean arterial pressure (MAP), pulmonary arterial pressure (PAP), and pulmonary capillary wedge pressure (PCWP) were monitored using a Hewlett-Packard Monitoring System 78354C (Hewlett-Packard GMBH, Boeblingen, Germany). Cardiac output was measured using the thermodilution technique (COM-2 Cardiac Output Computer, Baxter Healthcare Corp., Irvine, CA, U.S.A.) with simultaneous collection of systemic and pulmonary arterial samples.
Airway pressures were measured continuously using a Bicore CP-100 pulmonary monitor (Allied Health Care Products, Riverside, CA, U.S.A.). Plateau pressure (Pplat) was measured by occluding the expiratory valve for 3 sec while observing the pressure display to confirm stable pressure. Static compliance (Cst) of the respiratory system was calculated by dividing the effective tidal volume (VTeff) by the difference between Pplat and PEEP.
Induction of acute lung injury
After a stabilization period of 30 min, baseline data were recorded. ALI was induced by infusion of oleic acid, using a modification of method used by Suh et al. (17). Oleic acid 0.10 mL/kg (0.89 g/mL, Sigma Chemical, St. Louis, MO, U.S.A.), diluted 1:2 with absolute ethanol, was infused over a period of 30 min, into the right atrial port of the Swan-Ganz catheter with the animal in the supine position, and with a position change every 5 min. During induction of lung injury, Dextran-40 was administered to maintain a PCWP ≥ 6 mmHg. This was followed by a 90-min stabilization period before drawing the PV curve. If the arterial partial pressure of oxygen (PaO2) was greater than 300 mmHg after 60 min, an additional 0.02 mL/kg of oleic acid was injected over 1 min and re-evaluation was performed as described above. The experiment was not begun until adequate lung injury was evident (defined as PaO2 <100 mmHg on and after a 90-min stabilization period).
Pressure-Volume curve
Before initiating the experimental protocol for PEEP titration, the LIP was measured using the inspiratory PV curve. The inspiratory PV curves were determined using a modified multiple occlusion method (18). LIP was defined as the pressure at which the initial compliance line meets the maximal compliance line drawn on the PV curve (19). The PEEPINF was defined as the pressure set 2 cmH2O above the LIP of the PV curve.
PEEP titration
After the measurement of LIP, RM was performed by changing the ventilator setting to a CPAP of 50 cmH2O for 45 sec to move the lung physiology to the deflation limb of the PV curve. After RM, PEEP was increased to 20 cmH2O for 15 min, and then PEEP was decreased by 2 cmH2O every 15 min until the PaO2 was reduced by more than 10%, compared to the previous level of PEEP. The lowest level of PEEP that did not result in a significant drop (>10% of previous value) in PaO2 was defined as the PEEPDEF.
Thorax CT scan procedure
A thoracic CT scan was performed from the lung apex to the posterior costophrenic sulcus by use of a four-slice multi-detector CT scanner (Light Speed Advantage QX/i; General Electric Medical Systems, Milwaukee, WI, U.S.A.). Contiguous axial images with 10 mm thickness were reconstructed from the helical volumetric scan data (2.5 mm detector thickness, 10 mm beam collimation, beam pitch of 1:1.5, 120 kVp, 150 mA). CT data were obtained during an expiratory breath hold that was maintained automatically by use of a mechanical ventilator. The end-expiratory lung volumes (gas and tissue) were determined by use of a contiguous pixel method for the tissue, corresponding to the attenuation from +100 Hounsefield units (HU) to -1,000 HU as previously described (20). To differentiate lung zones with different degrees of aeration, the entire lung was divided into four zones as previously described (20): lung zones with an attenuation of less than -900 HU were considered as overinflated, those between -900 and -500 HU as normally aerated, those between -500 and -100 HU as poorly aerated, and those between -100 and +100 HU as nonaerated.
Experimental protocol
After obtaining PEEPINF and PEEPDEF, the animals were transferred to the CT unit. Using the same ventilator setting, except for the PEEP level, the animals were ventilated in a sequential manner with a PEEP of 0 cmH2O, PEEPINF, and PEEPDEF after RM (CPAP of 50 cmH2O for 45 sec). They were ventilated at each level of PEEP for 15 min, and at the end of this 15 min period measurements of lung mechanics, hemodynamics, and CT scans at end-expiration were carried out.
Statistical analysis
Data were analyzed using SPSS 11.0 (SPSS Inc, Chicago, IL, U.S.A.). Since the majority of the data were not normally distributed, all values were expressed as medians and interquartile ranges (25th and 75th percentiles) and the data were analyzed using nonparametric analysis. Therefore, nonparametric repeated measures analysis of variance (Freidman test) was performed to test for differences in each variable across the different levels of PEEP (21). When a significant difference was found among the three levels of PEEP, a post hoc comparison between PEEPINF and PEEPDEF was assessed using a Wilcoxon signed rank test. The significance of correlations between changes in PaO2 and changes in lung volumes was assessed using Spearman's coefficient (r). Two-sided p values <0.05 were considered to be statistically significant.
RESULTS
Baseline characteristics
Baseline characteristics of the animals are shown in Table 1. The median of PEEPINF was 13.4 (interquartile range, 12.5-14.3) cmH2O. PEEPDEF was evenly distributed from 10 cmH2O to 18 cmH2O, with a median of 12.0 (10.0-16.5) cmH2O, which was not significantly different when compared to PEEPINF (p=0.813) (Table 2). PEEPDEF was lower than PEEPINF in four animals, whereas PEEPDEF was higher than PEEPINF in two animals (Fig. 1).
Gas exchange
The PaO2 deteriorated significantly from 549.4 (494.0-596.4) to 88.4 (53.9-156.6) mmHg after induced lung injury at a PEEP of 0 cmH2O. After PEEP was increased to PEEPINF, the PaO2 increased to 438.8 (400.3-540.1) mmHg. At PEEPDEF, the PaO2 was 557.3 (485.6-593.2), which was also significantly increased when compared to PEEPINF (p=0.031) (Table 2). The shunt fraction was also significantly different between PEEPINF and PEEPDEF, with a median of 16.6%(9.3-24.2%) and 5.5% (3.5-9.3%), respectively (p=0.033) (Table 2). The PaCO2 was not significantly different between PEEPINF (80.6 [70.4-87.2] mmHg) and PEEPDEF (99.2 [81.1-108.9] mmHg) (p=0.066) (Table 2). There were no statistically significant differences in the pH between PEEPINF (7.13 [7.10-7.17]) and PEEPDEF (7.04 [6.93-7.17]) (p=0.062) (Table 2).
Compliance and airway pressure
After lung injury, Cst decreased significantly from 39.8 mL/cmH2O (33.9-44.6) to 17.2 (13.6-19.2). Cst at PEEPINF was 23.9 mL/cmH2O (18.8-29.0), not significantly different from Cst at PEEPDEF, which was 43.0 mL/cmH2O (16.2-56.9) (p=0.157) (Table 2). Also, there was no significant difference in Pplat between PEEPINF and PEEPDEF with a median of 20.0 cmH2O (20.124.1) and 16.5 cmH2O (13.729.3), respectively (p=0.562) (Table 2).
Hemodynamic variables
There were no statistically significant differences in MAP, PAP, or pulmonary vascular resistance between PEEPINF and PEEPDEF (Table 2). The cardiac index was significantly lower at PEEPDEF, with a median of 3.2 L/min/m2 (2.5-4.0) compared to PEEPINF, with a median of 4.3 L/min/m2 (3.0-5.4) (p=0.033) (Table 2). However, there was no statistically significant difference in oxygen delivery (DO2) between PEEPINF and PEEPDEF (p=0.065) (Table 2).
Lung volume on CT scan
CT scans obtained at a PEEP of 0 cmH2O showed large areas of consolidation in dependent portions of both lungs, and ground-glass opacity in the ventral lungs. When PEEP was increased to PEEPINF, this opacity was much decreased. CT scans obtained at PEEPDEF after RM showed better aeration in both lungs, when compared with scans obtained at PEEPINF (Fig. 2, 3).
The total lung volume at PEEPDEF was 2,000 mL (1,800-2,200), which was significantly higher than the 1,400 mL (1,300-1,700) of PEEPINF (p=0.035) (Fig. 4). The overinflated lung volume at PEEPDEF (20.7 mL [13.5-21.8]) was higher than PEEPINF (7.8 mL [5.4-10.9]) (p=0.035) (Fig. 4). The normally aerated lung volumes were significantly increased at PEEPDEF (1,395.2 mL [1,179.2-1,471.4]) compared to PEEPINF (843.1 mL [319.4-968.8]) (p=0.035); however, the nonaerated lung volumes at PEEPDEF (76.7 mL [56.2-93.5]) were significantly lower than that of PEEPINF (169.1 mL [97.6-378.1]) (p=0.035) (Fig. 4). There was no significant difference in the poorly aerated lung volumes between PEEPDEF (428.2 mL [352.6-878.9]) and PEEPINF (478.8 mL [453.0-577.4]) (p=1.0) (Fig. 4).
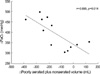
Correlations of the magnitude of the changes in PaO2 and respective lung volumes from a baseline PEEP of 0 cmH2O to PEEPINF and PEEPDEF were analyzed (2 data points per animal). There was a negative linear relationship between changes in PaO2 and the changes in poorly aerated plus nonaerated lung volume related to the PEEP changes (r=-0.685, p=0.014) (Fig. 5). There was no significant relationship between the changes in PaCO2 and the overinflated lung volume (p=0.618).
DISCUSSION
We evaluated the sequential effects of two clinically applicable methods of setting the PEEP level, one based on the LIP of the inflation limb of the PV curve (PEEPINF) and the other according to the oxygenation response during sequential decrements of the PEEP on the deflation limb following RM (PEEPDEF). The major findings of this study were that the PEEPDEF was associated with: 1) significantly increased oxygenation and decreased shunt fraction; 2) significantly increased normally aerated lung volumes and decreased nonaerated lung volumes; and, 3) significantly decreased cardiac index, compared to PEEPINF, although both had similar levels of PEEP.
PEEP recruits lung volume and prevents end-expiratory collapse of diseased lung, increasing the functional residual capacity (FRC); it thus improves oxygenation in patients with ARDS (7). Insufficient PEEP may result in alveolar derecruitment, cyclical atelectasis, progressive lung injury, and refractory hypoxemia (8). Excessive PEEP increase the risk of barotrauma and, particularly in combination with hypovolemia, can decrease cardiac output and oxygen delivery (9). However, the optimal way of setting PEEP in ARDS remains elusive, and up to now, many different approaches have been tried in attempts to optimize PEEP levels.
Recently, much attention has been given to use of the PV curve in setting PEEP levels in ARDS patients. Initially, most of the attention was focused on the inspiratory limb of the PV curve, with many studies using the LIP of the inflation limb as a guide for applying PEEP (12, 13). The use of this method has been associated with a decreased mortality and lower inflammatory response in ARDS patients (4, 5). The physiologic rationale for using LIP is that it reflects the pressure at which recruitment occurs and moves tidal ventilation to the linear portion of the PV curve (22). However, there are several limitations in using LIP to establish PEEP in ARDS patients. There are regional variations in LIP within the lungs of patients with ARDS (7), and alveolar recruitment actually occurs throughout inspiration, independent of the lower and upper inflection points, progressing from nondependent to dependent lung regions (23). In addition, alveolar derecruitment in ALI occurs over a wide range of pressures, and is poorly predicted by LIP (24). There are other logistical problems with using LIP for setting PEEP in patients with ARDS. LIP is difficult to measure and cannot be determined in some patients (25). In addition, chest wall mechanics can contribute to LIP, independent of alterations in lung mechanics (26, 27), and there is a large inter-observer variability in determining LIP (28).
Since PEEP can be considered to be an expiratory phenomenon designed to keep the lung open at the end of expiration, recent interest has focused on the other side of the pressure-volume curve, namely, the deflation limb of the PV curve. Rimensberger et al. reported that ventilation at a PEEP level above a critical closing pressure (determined by monitoring oxygenation and observing a decrease in PaO2 on the deflation limb after RM) resulted in a significant increase in end-expiratory lung volume and oxygenation and a decrease in lung injury (29, 30). Albaiceta et al. reported that the point of maximum curvature (PMC) of deflation limb of PV curve showed a significantly higher level of normally aerated tissue and a lower level of nonaerated tissue, when compared with the LIP in a CT scan study (16). However, Takeuchi et al. reported that a PEEP set at PMC showed no benefit in oxygenation and lung mechanics compared to using a PEEP set at the LIP+2 cmH2O (15).
The results of our study show that PEEPDEF is superior to PEEPINF with regard to maintaining lung volume and improving oxygenation, although in our study, both levels of PEEP appeared to be equally effective. In PEEPDEF, we wanted to develop a method of setting PEEP on the deflation limb of the PV curve, which is clinically applicable without the use of sophisticated devices (14). Although it is more ideal to use real lung volumes, accurate lung volumes can only be measured by body plethysmography, impedance plethysmography, or CT, which is currently only used in research investigations. Our study shows that since oxygenation is positively correlated with recruited volume (Fig. 5), using the PaO2 may be a clinically useful surrogate marker for recruited volume. The fact that Holzapfel et al. (10) found that the true expiratory inflection point (where curvature changes) correlates with the lowest PEEP level that achieves the maximum decrease in pulmonary shunting, lends support to our method of setting PEEP.
The results of this study are similar to another CT study that compared PEEP levels that were set according to both the inflation and deflation limbs of the PV curve. Albaiceta et al. showed that setting PEEP using the PMC of the deflation limb of the PV curve resulted in higher lung volumes and better oxygenation than did setting PEEP using the LIP of the inflation limb (31). However, in their study only data from three arbitrary slices of the CT scan were used for analysis. CT data acquired from a single slice, or even three, have been shown to be biased and to correlate poorly with data from the whole lung scan (32). We believe that this is the first study that has dissolved this issue using whole lung volumetric data.
In this study, PEEPDEF was higher than PEEPINF in some animals, while in others the reverse was true. While in some studies closing pressure of alveolar units has been suggested to be lower than the opening pressure (29, 33) , others have shown that the estimated closing pressure on the deflation limb of PV curve may be higher than LIP (15, 31). These conflicting results may reflect the heterogeneity of lung injury depending on the inciting agent and individual characteristics. This further adds to the argument that individual titration of PEEP may be important to recruit as much lung as possible while applying the least amount of pressure.
The fact that PEEPDEF had a higher overdistended lung volume compared to PEEPINF is of concern. However, the absolute increase in overdistended lung volumes was small (median, 8.1 mL) compared to the increase in normally aerated lung volume (median, 448.3 mL) or the decrease in nonaerated lung volume (median, 100.6 mL). The significance of this small increase in overdistended lung volume is not yet known, but it may contribute to increased dead space ventilation. Although, there was no significant difference in PaCO2 and pH between PEEPINF and PEEPDEF, there was a trend toward higher PaCO2 and lower pH at PEEPDEF. Also, there was a significant increase in PaCO2 and decreased in pH at PEEPINF and PEEPDEF compared to 0 cmH2O of PEEP, which could be interpreted as increased physiologic dead space ventilation due at least in part to increase in overdistended lung volumes. However, some of the increase in dead space might have been due to the increase in volume of air within the conducting airways (Fig. 2), and we could not find a significant correlation between change in PaCO2 and change in overdistended lung volumes. However, other studies have reported positive correlation between the volume of overdistended lung and PaCO2 (31, 34).
The decreased cardiac index seen at PEEPDEF compared to PEEPINF may be the consequence of higher lung volumes. Since an increase in pleural pressure in ALI is correlated with lung volume but not with airway pressure (35), the increased lung volume associated with PEEPDEF may have increased pleural pressure, thereby hindering venous return, which decreases venous flow, right ventricular stroke volume, and consequently cardiac output (36). This notion is supported by the fact that, on average, the PEEPDEF level (hence airway pressure) was actually lower than PEEPINF. This decrease in cardiac index may have been aborted with ample hydration, but in our protocol we did not give intravenous fluids other than maintenance fluids. Systemic vascular resistance, which is inversely related to cardiac output, may rise homeostatically to compensate for suboptimal cardiac output, helping to maintain an appropriate perfusion pressure across vital capillary beds. The increased systemic vascular resistance index seen at PEEPDEF compared to PEEPINF is likely to be related to this phenomenon.
The primary limitation of our study is the fact that it was performed on an oleic acid lung injury animal model with a small sample size. Thus, our data cannot be directly extrapolated to management of ARDS patients at this time. Since only six subjects were included, the study might have underestimated or overestimated the effect on different variables, including changes in lung volume or hemodynamic responses to PEEP changes. In addition, the order of PEEP applied was not randomized but sequential with PEEP based on inflation limb (PEEPINF) applied before PEEP based on the deflation limb after RM (PEEPDEF). Since volume history is one of major determining factors of lung recruitment, it is possible that the amount of recruitment we observed with our RM might have been influenced by prior ventilation at PEEPINF. However, since our goal was to compare method setting PEEP on the inflation limb of PV curve before recruitment and on the deflation limb of PV curve after near full recruitment, we believe sequential application of PEEP was adequate to address our question. Albaiceta et al. also used a similar approach in their CT study (31). Also, this was a short-term study, and it is not known what kind of long-term effect our method of setting PEEP might have on ALI patients. Furthermore, the mechanism of lung injury used in this study does not take into account the complex pathophysiology of human ARDS. Further studies are needed to compare the safety and effectiveness of two clinically applicable methods of setting the PEEP level in patients.






 XML Download
XML Download