

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Poisonings are the second most common cause of deaths related to injuries in Korea. It is associated with more than four thousand unexpected deaths and occupies 0.5 to 1.9% of emergency department (ED) visits per year (1).
According to the 2000 annual report of the American association of poison control centers (AAPCC) toxic exposure surveillance system (TESS), a total of 2,168,248 poisoned patients visited 63 poison control centers for one year in US. Among these patients, no toxicity was found in 818,323 (37.7%) patients, and only minimal toxicity in 1,082,047 (49.9%) (2, 3). The previous studies consistently reported that unnecessary ED visits due to poisonings may be reduced with the use of proper triage methods (4, 5). This reduction was accomplished, especially in children, over 50% (4). Those studies also suggested that a triage method should be developed for the efficient control of the out-of-hospital poisoned patients (5, 6). With the requirements aforementioned, 'the guideline for the out-of-hospital management of human exposures to minimally toxic substances' was approved in 2003 by AAPCC consensus panel (the AAPCC guideline) (3).
In Korea, there have been 12 local emergency medical information centers organized by the Ministry of Health and Welfare since 2000 (7). Each center collects real-time data from hospitals to obtain information on the availability of medical facilities through an automatic report system, and provides emergency medical advices to the lay persons who are in trouble. The Seoul Emergency Medical Information Center (SEMIC) is responsible for Seoul, which is the largest city in Korea, and 10,276,968 people live in (8). Four physicians with 12 emergency medical technicians (EMTs) are working at the SEMIC as emergency medical advisers. They provide guidance of emergency care and information relating hospital data, which were required to the out-of-hospital patients, to callers. The SEMIC collects data from 61 medical institutes in Seoul and receives more than 70,000 calls from lay persons per year (7). The calls relating out-of-hospital poisonings occupy 0.5% of the total calls. Until now, however, there has been neither triage method nor toxic exposure surveillance system for the out-of-hospital poisoned patients.
The aim of this study was to develop and evaluate a triage method to prevent the unnecessary ED visits of out-of-hospital poisoned patients.
MATERIALS AND METHODS
Study design
This study was a prospective, observational study using a triage protocol with reference to the AAPCC guideline for out-of-hospital poisoned patients (3). The Seoul National University Collage of Medicine/Seoul National University Hospital Institutional Review Board reviewed our investigation and article.
Study setting & population
From October 2003 to September 2004, telephone calls that lay persons gave to the SEMIC to seek advices of us on poisoned patients were enrolled. Exclusion criteria were the calls that were not able to offer adequate histories due to hang-up or inappropriate communication or the calls that were not able to offer medical outcome during follow-up procedures (3). When the responders of SEMIC decided that the patient had a critical situation requiring prompt resuscitation, they ordered the caller to start resuscitation without delay and excluded the case from this study.
Study protocol
We designed a triage protocol consisted of five factors and applied it to the patients who were consecutively enrolled during the study period (Fig. 1). We used the list, 'the examples of minimally toxic substances approved by the AAPCC panel', to distinguish minimally toxic substances from other toxic substances (3). We also used four factors to decide patient's disposition on the basis of the AAPCC panel's suggestion, which were patient's intent, symptoms or signs, social environment, and individual patient circumstances (3).
From the histories, we found out the identity of the substances involved in the exposures, estimated the maximum amount of the substances, and secured the symptoms or signs that the patients complained of (3). To identify the ingredients of substances, we investigated web or references recommended in the guideline (3). If we failed to identify the ingredients of substances, we regarded the substances as toxic. We regarded only the substances that were implicated in the list as minimally toxic (3).
According to the protocol, we divided the patients into the two groups, the high-risk group and the low-risk group (Fig. 1). Then, we recommended an immediate ED visit to the patients in the high-risk group and recommended a close-observation in pre-hospital state to the patients in the low-risk group. To prevent adverse effects, we also recommended they should visit ED as soon as possible, if the patients in the low-risk group were in trouble during a period of observation (9).
Measurements
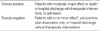
Nine EMTs of SEMIC were educated on the protocol for 4 hr and obtained the histories of patients from callers according to the data table of TESS reports (10-13). Table 1 shows medical outcomes. To acquire the medical outcomes of the patients, follow-up procedures were performed. We made a telephone call to the caller within 3 months after the initial call. If we had failed to connect the caller or acquire the medical outcome of the patient from the caller till 3rd trial, we regarded the case as the follow-up failure and excluded it from this study. According to the medical outcomes, we assigned the patients to the two groups, the toxicity-positive and the toxicity-negative.
Data analysis
To determine of the priority of the factors in the triage protocol, we calculated the odds ratio (OR) of each factor for the toxicity-positive using chi-square test and Fisher's exact test of the SPSS 11.0 for Windows. On the basis of the priority, we developed a flow chart as a triage method. We also calculated the sensitivity, specificity, positive predictive value and negative predictive value of the method. We regarded the value of specificity as the ability to reduce of the unnecessary ED visits in the toxicity-negative group, and the value of sensitivity as the safety of the method to recommend no ED visit in the low risk group.
RESULTS
From October 2003 to September 2004, a total of 292 calls to seek the medical information relating poisoned patients were given to the SEMIC by lay persons. Twenty six calls (8.9%) were not able to offer adequate histories. Of these calls, hang up were nineteen calls (73.1%) and inappropriate communication were seven calls (26.9%). One call (0.3%) required prompt resuscitation and we failed to obtain adequate histories from the caller. Forty five calls (15.4%) were regarded as follow-up failure by us. During the follow-up procedures, we failed to contact the caller in 32 calls (71.1%), and we failed to obtain medical outcome from the caller in 13 calls (28.9%). Finally, two hundred twenty calls (75.4%) were included in this study and each call was attributable to a separate case.
Table 2 and 3 display the obtained histories from the callers. Table 4 shows the ORs of the five factors for the toxicity-positive in the triage protocol. Fig. 2 shows the flow chart as a triage method according to the priority of ORs of the five factors. The value of sensitivity and specificity of the triage method was 99.2% and 53.4%, respectively (Table 5). False negative case was shown in only one patient (1/48).
The patient was a 32-yr-old male and exposed to small amount of Madecassol ointment by ingestion. After five minutes of the exposure, he made a call to the SEMIC without any symptoms or signs. The EMT of SEMIC classified him as the lower risk group and recommended to stay at home with observation. About 30 min later, he felt abdominal pain and visited an ED. With an infusion of fluid and pain killer, abdominal pain was subsided. He was discharged from the hospital and did not complain of any more symptoms or signs.
Of the 172 patients in the high-risk group, 41 patients (23.8%) were assigned to the toxicity-negative. Table 6 illustrates the causes of these false positives.
DISCUSSION
The primary goals of the AAPCC guideline are to establish principles to aid in identifying a minimally toxic substance, to provide examples of substances that meet the principles, and to provide an approach to adding additional substances to the list (3). It is the first standardized guideline for the triage of the out-of-hospital poisoned patients and composed of methods of data collection, a definition of minimally toxic substances, a consensus of the guideline, a process to determine if a substance should be added to the minimally toxic list, and a need of follow-up procedures (3). In the guideline, on the assumption that all substances are capable of producing toxicity and nothing is completely non-toxic, the panel defined the minimally toxic substances as those which produce little toxicity, minor self-limited toxicity, or clinically insignificant effect at most doses (3). After going over literatures and taking into account the expert opinions of its members, the panel selected 30 examples of minimally toxic substances and then approved 25 among them (3). In the guideline, the panel also suggested that the decisions regarding patient disposition should take into account the patient's intent, symptoms, social environment, and individual patient circumstances (e.g., pregnancy, pre-existing medical conditions, and current medications) (3). Of these contents of the guideline, we cited the minimally toxic list and the factors that should be considered in decisions regarding patient disposition because the aim of this study was to develop and evaluate a triage method for the out-of-hospital poisoned patients (Fig. 1).
The sensitivity and the negative predictive value of the triage method were 99.2% and 97.9%, respectively (Table 5). It means that the high-risk group designation predicts almost all the toxicity positive patients. This method can be used safely. The specificity and the positive predictive value of the method were 53.4% and 76.2%, respectively (Table 5). It means that this triage method is able to reduce more than a half of the unnecessary ED visits of the out-of-hospital poisoned patients. However, the specificity and the positive predictive value of the method were not so high. It might be an inevitable result in this study. Since it is impossible to provide direct physical examinations or immediate therapeutic interventions to the poisoned patients by telephones, it is very important to reduce false negatives (3-5, 14).
Madecassol ointment was the only one substance caused false negative in this study. It is composed of Centella asiatica products, neomycin, and hydrocortisone and it is categorized into 'corticosteroids, topical with antibiotics' (15). According to 'the examples of minimally toxic substances approved by the AAPCC panel', it is included in the minimally toxic substances (3). In a few cases, however, the Madecassol ointment ingestion has been reported to disturb digestive system and cause gastrointestinal symptoms, which would be fully recovered with appropriate therapies (15, 16).
The most common cause of the false positives was the substances regarded as toxic (Table 6). More substances should be identified as minimally toxic for the reduction of false positives, through the process proposed by the AAPCC panel, involving a review of current literatures, a thorough analysis of poison experience, and prospective validation (3).
We designed this protocol with reference to the AAPCC guideline and collected data according to the data table of TESS reports (2, 3, 11-13). However, there were some limitations addressed in the AAPCC guideline and TESS. Firstly, drug identification principles were not developed. Drug identification practices varied from center to center throughout the United States and amount estimation depended on the histories obtained from callers (5, 17). Secondly, the optimal sources for the outcome were not established (3, 5). The TESS data recognized several different toxic effects as the medical outcome categories (10). However, the data had inherent limitations and using them alone was problematic and not satisfactory (3). Additional data sources were required for the medical outcome to provide an accurate perspective on the feasibility of the triage method (3). For the additional data sources, we obtained more information during follow-up procedures on ED visits, therapeutic interventions, and hospital admissions.
In addition to the above limitations, there were other limitations in this study. Firstly, the distribution of the study population inclined toward the patients acutely exposed in safe environments. Most of the calls were given to us by the family members at home (Table 2). In other words, most of the patients were located in safe environments where their family members could take care of them. In addition, chronically exposed patients were not included (Table 2). Since most of the chronically poisoned patients had no idea of poisonings, they called us not to obtain information on poisonings but to obtain information on other problems, such as chronic headache, chronic diarrhea, depression, or others. Initially, we could not recognize them as poisoned patients and failed to apply the protocol to them. Secondly, all exposures occurred in the restricted region, Seoul. Compared with 2003 annual report of the AAPCC TESS, most of the demographic findings of this study were similar to those of the report, but the substances commonly involved in exposures of the two were different (Table 3) (13). Many studies reported that the nature of exposure in one region can differ from that of another, and the difference is determined by the regional environmental factors (17, 18). However, the EMTs of SEMIC provided advices to the persons lived in Seoul, and they could not obtain information on toxic exposures occurred in other regions than Seoul in this study. Finally, we failed to identify the ingredient of herbs, Korean traditional herbal remedies. Most of the herbs are composed of several unknown plants and we were not able to find any reference in the ingredient of the herbs. In this study, nine (4.1%) patients took the herbs and five (2.3%) were intoxicated. The composition and the toxicities of herbs should be identified through the process proposed by the AAPCC panel (3). Despite these limitations, this study was the first trial to develop and evaluate a triage method to prevent unnecessary ED visits of out-of-hospital poisoned patients, with reference to the AAPCC guideline.
Our triage method with reference to 'the guideline for the out-of-hospital management of human exposures to minimally toxic substances' approved by the AAPCC consensus panel prevented more than half of unnecessary ED visits of out-of-hospital acutely poisoned patients, safely.







 XML Download
XML Download