

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Current evidence indicates that chronic subclinical inflammation may play an important role in the genesis and progression of atherosclerosis, and many recent reports have explored the association between C-reactive protein (CRP) levels and atherosclerosis. CRP is present in the acute reaction phase of inflammation, and elevated levels of serum CRP are related to a poorer outcome in patients with cardiovascular diseases (1, 2).
Several studies have suggested that CRP is a predictor of subsequent cardiovascular events in healthy adults (3). Recently, high-sensitivity C-reactive protein (hs-CRP) has emerged as a useful biomarker for vascular inflammation associated with atherosclerosis. While a significant amount of data has been amassed about vascular disease in adults, limited data exists concerning the low grade inflammation in obese children. Because atherosclerosis frequently begins in childhood, we assessed the association of two markers of early atherosclerosis, serum hs-CRP level and atherosclerotic risk factors with carotid intima-media wall thickness (IMT) and brachial flow-mediated dilation (FMD) in obese children.
MATERIALS AND METHODS
Subjects
The study subjects were 83 children. Thirty-eight children were obese (14-16 yr of age, male), and 45 were sex/age-matched healthy control children. All were nonsmokers without any regular medication and had no family history of premature vascular disease. None of the children had symptoms of infection during the 2 weeks before the study.
Anthropometric measurement and clinical examination
Body height and weight were measured in light clothes using a portable standiometer. Body mass index (BMI) was calculated as weight divided by the square of the height (kg/m2). In children, the 95th percentile for BMI in the 2000 CDC growth chart is 21-23 (4), so we used BMI >23 as our prospectively defined criterion for obesity, and BMI <21 was defined as the non-obese control level.
Serum lipids and apolipoprotein
Venous blood samples were taken in the morning after overnight fasting (10-12 hr). Serum total cholesterol (TC), low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), and triglyceride (TG) concentrations were measured by standard enzymatic methods with the use of Boehringer Mannheim GmbH and a fully automatic analyzer. Serum apolipoprotein A-1 (Apo A-1), apolipoprotein B (Apo B), and apolipoprotein E (Apo E) were measured by immunonephelometry (Behring Nephelometer II, Dade Behring, Inc., Newark, DE, U.S.A.).
High-sensitivity C-reactive protein
A BN II Nephelometer Analyzer (Dade Behring, Inc.) was used to measure serum hs-CRP values using a high sensitivity latex-enhanced immunonephelometric assay method. The detection limit of this assay was 0.17 mg/dL. Because the 90th percentile of normal CRP distribution is 0.3 mg/dL, we included only patients with CRP values below 0.3 mg/dL to avoid the influence of acute infection.
Ultrasound studies
All ultrasound studies were performed in the morning on fasting subjects with the use of Hewlett-Packard Sonos 5500 and a 3-11 MHz linear array transducer (Philips, Andover, Massachusetts, U.S.A.). All ultrasound scans were performed by an experienced vascular operator who was unaware of the children's clinical details. Blood pressure was measured from the brachial artery of the nondominant arm 3 times during the ultrasound study with the use of a standard sphygmomanometer, and the mean value of these 3 measurements was used for the analyses. The brachial artery evaluations and carotid artery evaluations were performed by using standard techniques for the study of children.
Brachial artery evaluation
Brachial artery diameter was measured during reactive hyperemia from B-mode ultrasound images at rest. The subjects lay quietly for 10 min before the first scan. The brachial artery was scanned in a longitudinal section 5 to 15 cm above the elbow. Depth and gain settings were set to optimize images of the lumen-arterial wall interface, and the operating parameters were kept constant during the study. A resting scan was performed, and the arterial flow velocity was measured using a Doppler signal. Increased flow was then induced by inflation of a pneumatic tourniquet placed around the forearm (distal to the scanned part of the artery) to a pressure of 250 mmHg for 5 min, followed by release. Subsequent scans were taken continuously for 60 sec after cuff deflation. We also included a repeated flow velocity recording for the first 15 sec after the cuff was released. Vessel diameter was measured by an experienced reader who were blind to the study subjects' laboratory data. The arterial diameter was measured at a fixed distance from an anatomic marker with the use of ultrasonic calipers. Measurements were taken from the anterior to the posterior M line at end diastole, incident with the R wave on a continuously recorded ECG. The maximal proportional dilatation from baseline (FMD) was assessed.
Carotid artery analysis
Carotid artery IMT measurements were done according to a predetermined, standardized scanning protocol for the right carotid artery. Briefly, the proximal part of the carotid bulb was identified and the segments of the common carotid arteries 1 to 2 cm proximal to the bulb were scanned. The image was focused on the posterior wall, and the resolution box function was used to magnify the arterial far wall. All scans were digitally stored for subsequent offline analysis. One end-diastolic frame (captured adjacent to the R wave on a continuously recorded ECG) for each interrogation angle was selected and analysed for mean IMT. Five measurements for far wall IMT were taken manually for each image using ultrasonic calipers, and the average values of these readings were used for the analyses.
Statistical analyses
SPSS version 11.0 was used for all statistical calculations. Results were expressed as mean±standard deviation. Comparisons between two groups were performed by the independent student-t test. Univariate and multivariate regression analyses were used to dclineate the relationships between arterial changes and CRP. Due to the skewed distribution of hs-CRP levels, CRP values were logarithmically transformed prior to regression analyses. For all analyses, probability (p) values below 0.05 were considered statistically significant.
RESULTS
Clinical characteristics
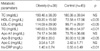
Height and weight were significantly higher in the obesity group than in the control group. BMI was 29.40±3.18 kg/m2 in the obesity group and was 18.43±1.00 kg/m2 in the control group (Table 1). Obese children had significantly higher systolic blood pressure (SBP) (133.05±8.84 mmHg vs. 115.16±8.62 mmHg), diastolic blood pressure (DBP) (84.95±9.02 mmHg vs. 75.16±6.92 mmHg), hs-CRP levels (0.10±0.07 mg/dL vs. 0.06±0.04 mg/dL, p<0.01) and significantly higher LDL-C, TG, Apo B and lower HDL-C than the control group (Table 2). TC and Apo E were higher and Apo A-1 was lower in the obesity group than in the control group, but these differences were not statistically significant.
Ultrasonic findings
Obese children were also found to have increased IMT (0.52±0.09 mm vs. 0.40±0.07 mm, p<0.001) and impaired FMD (7.35±7.78% vs. 20.34±16.81%, p<0.001) compared to healthy controls (Table 3).
Relationships between IMT, FMD and atherosclerotic risk factors
IMT correlated with BMI (r=0.612, p<0.001), SBP (r=0.510, p<0.001), DBP (r=0.307, p<0.05), and HDL-C (r=-0.221, p<0.05). FMD correlated with BMI (r=-0.414, p<0.001), SBP (r=-0.437, p<0.001), TG (r=-0.445, p<0.05), and Apo E (r=-0.402, p<0.05) (Table 4).
Relationships between hs-CRP and atherosclerotic risk factors
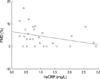
Log [CRP] showed a positive correlation with BMI (r=0.470, p<0.001), SBP (r=0.209, p<0.05), DBP (r=0.230, p<0.05), Apo E (r=0.308, p<0.01), and TG (r=0.288, p<0.05) by simple regression (Table 5).
DISCUSSION
The present study showed that elevated serum CRP levels were significantly associated with endothelial dysfunction and increased carotid artery IMT in obese children. While there have been many previous studies relating CRP and cardiovascular risk factors (5, 6), the association of CRP with subclinical atherosclerotic findings has been examined primarily in adults, with few studies in obese children (7, 8).
Historically, CRP has been measured in clinical laboratories by immunoturbidimetric and immunonephelometric assays designed to detect active inflammation and infection. The dynamic range of these assays is from 3 mg/L (90th percentile of the general population) to well over 200 mg/L. Although such assays are automated and reproducible, they have a relatively low detection limit of 3 to 8 mg/L and thus do not have appropriate sensitivity in the range required for the determination of cardiovascular risk (9). To achieve the desired limit of quantification, hs-CRP assays have been developed that can reliably measure hs-CRP concentrations as low as 0.15 mg/L (<2.5th percentile of the general population). When measured with a high-sensitivity assay, CRP levels appear to have a predictive value for cardiovascular morbidity and mortality. Moreover, baseline levels of CRP predict the risk of future myocardial infarction, stroke, and peripheral atherosclerosis, even after adjustment for other known cardiovascular risk factors (10). We employed this method in the present study, and we found that obese children had significantly higher hs-CRP levels than control subjects. Further studies will be required to determine cut-off values for hs-CRP in obese children.
High-resolution ultrasound is a reliable, noninvasive method for detecting early structural and functional atherosclerotic changes in the arterial wall. Increased carotid IMT is a structural marker of early atherosclerosis that correlates with vascular risk factors and is related to the severity and extent of coronary artery disease. FMD of the brachial artery is a marker of endothelial function that can be assessed by measuring arterial diameter responses to increased flow (11). Brachial artery FMD occurs mainly as the result of endothelial release of nitric oxide and correlates with coronary endothelial function (12). Both increased IMT and impaired FMD have been detected in young children who have risk factors for atherosclerosis such as familial hypercholesterolemia (13) and diabetes (14). In the present study, obese children were also found to have increased IMT and impaired FMD compared to the healthy controls. In addition, IMT was positively correlated with BMI, SBP, and DBP, and negatively correlated with HDL-C concentrations. Zhu et al. reported a similar result in 43 obese children (15), and Kim et al. showed that IMT correlated with DBP and homocysteine concentrations (16).
Woo et al. have confirmed that the degree of endothelial dysfunction correlated with BMI as assessed by multivariate analysis (17). In the current study, FMD was shown to correlate with BMI, SBP, and TG and Apo E concentrations.
Traditional risk factors for cardiovascular disease include aging, hypertension, dyslipidemia, smoking, and diabetes. The contribution of lipid accumulation to atherosclerotic disease is well known, but laboratory and experimental evidence indicates that chronic inflammatory processes also play an important role in the development of atherosclerosis (18). In order to effectively prevent the incidence of cardiovascular events, it is important to weigh the influence of each risk factor on the cardiovascular system. In addition, it should be borne in mind that various cardiovascular factors are not independent of one another but often have direct or indirect interactions (19). In this respect, we investigated the relationship of inflammatory markers with other risk factors. Elevated serum CRP levels were positively associated with elevated BMI, confirming previous observations in both children (19) and adults (20). The mechanisms underlying this association with BMI or obesity might be as follows; the adipose tissue is a source of cytokines such as tumor necrosis factor-a (TNF-a) and interleukin-6 (IL-6), and these cytokines stimulate the production of acute-phase proteins such as C-reactive protein in the liver (21). Not unexpectedly, then, we found that serum CRP levels were positively associated with BMI. Because we have not checked proinflammatory cytokines such as TNF-a and IL-6, we can not verify the elevation of these cytokines as a consequence of obesity.
In addition to BMI, CRP was also found to be closely correlated with SBP, DBP, and ApoE and TG concentrations. Previous studies reported that CRP levels are significantly positively correlated with TG, total ratio of serum cholesterol to serum HDL cholesterol (22), fibrinogen levels, heart rate, SBP (19), smoking, and white blood cell count (5) and negatively correlated with HDL-C levels (19, 22). Several studies have examined the relationship between CRP and carotid IMT in adults. Hak et al. found a highly significant relationship between markers of obesity and CRP in healthy, middle-aged women, but failed to find a significant relationship between CRP and subclinical atherosclerosis of the carotid system (20). Sitzer et al. performed a large scale study that showed the serum CRP level is linearly positively correlated with IMT in apparently healthy adults (3). Hayaishi et al. reported that the hs-CRP level is positively associated with carotid IMT in young patients with type 1 diabetes (23). Several studies have also shown an association between elevated CRP concentrations and endothelial dysfunction in adult patients with coronary artery disease (24) and with type 2 diabetes (25). In contrast to the significant amount of data that has accumulated from adult individual, limited data exists concerning CRP and subclinical atherosclerosis in children. Jarvisalo et al. reported that, in healthy children, elevated serum CRP levels were significantly associated with decreased endothelial vasodilatory function and increased IMT (26). Our results are consistent with the Mangge's report (27) that serum hs-CRP correlated positively with IMT and inversely with FMD in the obesity group. In other words, if hs-CRP is increased in asymptomatic obese children, we can assume the existence of and advanced subclinical atherosclerosis, increased IMT, and decreased endothelial vasodilatory function without performing an ultrasound.
In summary, we found a highly significant correlation between the serum CRP concentration and the early stage of atherosclerosis in obese children. Although ultrasonography allows visualization of early subclinical stages of atherosclerosis in obese children, the measurement of the serum hs-CRP level is simpler and cheaper than ultrasonography, is highly reproducible, and well correlates with IMT and FMD in obese children. Thus, hs-CRP would be a useful screening marker for evaluating and estimating the degree of atherosclerosis in children.





 XML Download
XML Download