

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Congenital cyst of pancreas is a very rare lesion, usually seen in female fetuses, which could be detected with prenatal ultrasonography (US). It needs to be differentiated from mesenteric cyst, lymph node cyst, ovarian cyst, and multiple cysts of the kidney in fetal life.
CASE REPORT
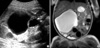
A 23-yr-old woman to be in gravida 3, para 1 was referred to the Chosun University Hospital due to a cyst in the abdomen of fetus on routine US from private clinic. We performed ultrasound which showed a 56×47 mm cyst suspected to be a mesenteric cyst or ovarian cyst (Fig. 1A). The size of the cyst did not change during follow up US and the fetus showed a normal development. Spontaneous labor was at 38 weeks' gestation. The healthy female neonate weighing 3.6 kg with 49 cm height was born via spontaneous vaginal delivery. The newborn was admitted to nursery after birth to examine the cyst observed through prenatal US and underwent routine biochemical, hematologic tests, chromosome study and MRI. The biochemical, hematologic and chromosome studies were normal. MRI revealed a 56×47 mm homogenous cyst in the right posterior retroperitoneal space. This cyst showed low signal density on T1 weighed images and high signal intensity on T2 weighted images (Fig. 1B). No enhancement was seen after the use of intravenous contrast enhancer. This cyst was pressing against the tail of pancreas and inferior vena cava. The neonate underwent surgery to remove the cyst. The excision of the cystic mass originating from the pancreatic tail was performed with distal pancreatectomy (Fig. 2). The cyst contained amylase (30 U/L). Gross examination of the cyst showed a 8×8 cm fresh cyst containing clear fluid inside. In immunohistochemical stains, calretinin and CD 34 were negative and cytokeratin was positive (Fig. 3B). The histopathologic diagnosis was pancreatic cyst. The baby recovered well after operation.
DISCUSSION
Congenital pancreatic cyst is a rare lesion in the neonatal period (1). Embryologically, they arise from a developmental anomaly of the pancreatic ductal system and usually originate from the pancreatic body and tail. True pancreatic cyst contains a true epithelial tissue not seen in pseudo-pancreatic cyst developing after trauma or infection (2). It is usually seen as solitary, unilocular, nonenzymatic, and fill with sterile fluid. The cyst composes of normal pancreatic tissue without any inflammatory response. True congenital pancreatic cyst is complicated with infection and inflammation in some cases, and it brings difficulty in diagnosis (1). It could be seen as multiple cysts if they accompany with Beckwith-Wiedmann syndrome (3), polycystic disease of the pancreas and kidneys (2), and von Hippel-Lindau disease (4). It may also associate with tubular ectasia, polydactyly, anorectal malformation, and asphyxiating thoracic dystrophy. In most cases, true pancreatic cysts do not change the sizes during pregnancy. However, Kebapci et al. (6) reported that a pancreatic cyst changed in the sizes almost 12 times after birth, pressuring the adjacent viscera. Unilocular cyst can change to multilocular cysts in some cases.
Clinically, congenital pancreatic cyst is asymptomatic or accompany with polyhydramnios. After birth, symptoms are revealed as abdominal mass, abdominal distention, nausea and jaundice due to bile duct obstruction (1, 4). Congenital pancreatic cyst looks like soft tissue mass between the stomach and transverse colon on plain radiography. Ultrasound or computerized tomogram or MRI images show detailed information including the characteristics of the wall, septum, internal structure and surrounding tissues. However, it is very difficult to differentiate pancreatic cyst from other abdominal cysts during fetal life or neonate. The diagnosis of congenital pancreatic cyst should be differentiated from liver and choledochal cysts, mesenteric cysts, meconium pseudocysts, dilated bowel, urachal cysts, gastrointestinal duplication cysts, hydroureteronephrosis, cysts of the renal origin, multiple dysplastic kidney, ovarian cysts, and hydrometrocolpos (5). Congenital pancreatic cyst is treated differently according to their site of origin. The cyst developed in the pancreatic body or tail can be surgically removed by total excision. Internal drainage is done for those cysts developed in the head of the pancreas (2).
Physicians need to consider the possibility of a congenital pancreatic cyst when a large abdominal cyst is present in a fetus or neonate. Prenatal US is effective in detection of the fetal pancreatic cyst and following up the size. The complications of fetal pancreatic cyst are infection within the cyst, infection of the bile duct, rupture of the cyst, and peritonitis (6, 7).


 XML Download
XML Download