

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Up to date, numerous studies have found important predictors associated with the prognosis of alcohol dependents. It has been known that better outcomes of alcoholics are related to the various factors such as less severity of alcohol dependence (1, 2), old age (3), higher cohesiveness of family (4), late onset of alcoholism (5, 6), absence of genetic trait (6), etc. However, it is more important to find the factors that can be improved by therapeutic effort. Project MATCH research group (7) indicated that alcoholics' motivation and social support are important changeable factors influencing prognosis, and suggested that treatment focusing on these targets is required.
One of the intrinsic factors that can be enhanced by therapeutic efforts is the level of patients' insight, which can be an important element in induction of motivation for treatment and behavioral change. However, alcohol dependents who are deficient in insight account for 84.3-94.7% of patients in touch with therapeutic systems in Korea (8-10). Lack of alcoholics' insight is one of the most common barriers to treat alcoholism in Korea.
A body of research has focused on the relationships between alcoholics' insight and the factors related to diagnosis and treatment process. False negative results are frequently encountered in alcoholism screening test specifically for those with lower levels of insight (11). Thus, it is suggested that caution for the level of insight should be taken with the interpretation of alcoholism screening tests. The results of the studies that the treatment programs for inpatients were of considerable help in the enhancement of alcoholics' insight (8, 11, 12) indicated that the insight of the alcoholics is a factor that can be modified by the therapeutic efforts. Kim et al. (9) revealed that the various defensive mechanisms commonly used in alcoholics such as acting out, denial, show-off, and somatization are different according to patients' insight levels. The assertion that the level of alcoholics' insight plays an important role in the process of recovery is supported by the report that it is associated with treatment compliance (13).
Evaluation of insight is part of mental state examination. Sadock (14) classified patients' insight levels into impaired, intellectual and true insight, according to the degree of insight formation. Kim (15) proposed five focuses as the components required in the evaluation of alcoholics' insight. At a theoretical level, it may not be remarkably surprising that patients with a better understanding of their alcoholism have a better outcome. However, as with the exact role and function of insight on their outcomes, it was poorly understood in the clinical field of alcoholism. The present study was performed to examine the relationship between the abstinence results of alcohol dependents after discharge and their insight level at the time of discharge.
MATERIALS AND METHODS
Subjects
The subjects were male Korean alcohol dependents discharged from a community-based alcohol treatment center, who had been diagnosed under DSM (Diagnostic and Statistical Manual of Mental Disorders)-IV criteria (16) as alcohol dependents without other forms of drug abuse/dependence. Among the 151 consecutive admissions for 1 yr, 28 patients who were unsuitable as follow-up subjects were excluded; 3 died during the hospitalization, 2 with symptoms of cognitive impairment, 8 with other forms of psychiatric diagnosis, and 15 transferred from municipal social isolation facilities available for homeless, or the like for temporary medical service. Written and informed consents were obtained from 123 patients after thorough explanation about the study was given. This study was approved by the Ethics Committee of the Chungnam National University Hospital.
Data collection procedure
In the early admission period, usually within 1 week after admission, baseline data of the patients who passed through withdrawal symptoms were collected by face-to-face interviews lasting approximately 1 hr using a structured interview schedule that consisted of both interviewer- and self-report portions about pretreatment participant socio-demographic, drinking-related and family history, and insight state. One day prior to the prospective discharge, patients' insight states were evaluated again.
Demographic characteristics such as age, educational state, type of occupation and religion, and marital state were included in baseline data collection. Environmental support for patient's abstinence was assessed by the presence or absence of dissuasion from patients' drinking by family and colleagues. Family functioning (17, 18), family adaptability and family cohesiveness (19) were examined.
The score of lifetime alcohol-related consequences (20) that is one of the most widely used measures for assessing alcoholism was investigated. Age of first drinking, duration of drinking problems and prior experiences of admission treatment due to drinking problems were examined. Drinking behavior was assessed through drinks per drinking day and drinking days in 1 month prior to admission. Patients marked the drinking days and the types and sizes of Korean beverage they consumed on the calendar. Quantity of drinking was then converted to standard drinks (12 grams of alcohol/drink).
Collection of follow-up data was planned to occur every 2 weeks during the first month and monthly from the second month to the twelfth month after discharge from the hospital. Post-discharge interviews were encouraged to occur in the scheduled appointments by facilitating aftercare visits, family interviews and telephone interviews. Re-admission interviews replaced the post-discharge interviews in the readmission cases due to relapse. During each post-discharge interview, the drinking days on the calendar and types and size of Korean beverage consumed in the inter-interview days were investigated. The criterion for abstinence in this study was set as the total absence of drinking behavior. Initial months of abstinence on a successive basis after discharge (IMA), total months of abstinence during 1 yr after discharge (TMA) and complete abstinence for 1 yr were used for the analysis of abstinence results.
Insight-evaluating measure
The 20-item Hanil Alcohol Insight Scale (HAIS) (21) was used for evaluation of patients' insight state. The HAIS (Table 1) was designed to ask four times in different combinations about each of the areas of insight to get quantitative and qualitative information of insight. The questions reflecting the positive direction of insight involve questions 1, 3, 5, 7, 9, 12, 14, 16, 18, 20 and negative direction, questions 2, 4, 6, 8, 10, 11, 13, 15, 17, 19. Those with intellectual nature of insight involve questions 1, 2, 3, 4, 5, 11, 12, 13, 14, 15 and emotional, questions 6, 7, 8, 9, 10, 16, 17, 18, 19, 20. Concurrent validity study (21) of HAIS showed high correlation (r=0.79, p<0.001) with 3 clinicians' judgments, and the sensitivity of 76.9-100% and specificity of 83.3-94.9% for the classification of the insight state of 44 male patients who were labeled as having the same level (poor, fair and good) of insight from interviews by three clinicians in charge of the alcoholism treatment programs. Considering the mean and standard deviation of insight scores of 3 groups classified by insight level, it was recommended that the patients with scores of -20 to 3 should be interpreted as having poor insight, 4 to 15 as fair and 16 to 20 as good on the basis of total score (21). The reliability indices for the item showed a significant item-total correlation over all 20 items (p<0.01) (8), with Cronbach's alpha of 0.82-0.89 (8, 13, 21), Spearmen-Brown half-split coefficient of 0.73-0.91 (8, 21), Guttman half-split coefficient of 0.73 (21), and a significant (p<0.001) test-retest correlation (21).
Data analysis
Baseline characteristics of 3 groups based on insight level were compared by chi-square test and ANOVA with LSD or Dunnett's T3 post hoc analysis. The mean IMA and TMA of 3 groups according to insight level were compared by ANCOVA for the control of the differences in baseline characteristics across the insight levels. For an analysis of complete abstinent patients for 1 full year after discharge, logistic regression test with adjustment for the differences in baseline characteristics across the insight levels was performed. The rates of patients continuously abstinent in 3 groups based on insight level at each month during the follow up period were compared by 1-month stepwise life table analysis. p values lower than 0.05 were used as criteria of statistical significance level.
RESULTS
6 patients (4.9%) dropped out because 3 died during the follow-up period and 3 were missed due to failure to remain in contact. 117 patients who had been followed up had a mean (SD) insight score of 5.83 (8.15) at admission and 8.91 (7.57) at discharge and 6 drop-outs had a mean (SD) of 4.50 (10.06) at admission and 12.67 (6.28) at discharge, with no significant difference in insight score between the two groups (t=0.387, 121 df, p>0.05 at admission, t=1.192, 121 df, p>0.05 at discharge). 117 patients were distributed into 31 in poor, 58 in fair and 28 patients in good insight by their insight score at discharge. The mean (SD) frequency of post-discharge interviews in 117 patients was 10.13 (2.76), and it was not significantly different among the insight levels; 9.26 (3.02) in poor, 10.66 (2.66) in fair, and 10.00 (2.47) in good insight patients.
Table 2 displays baseline characteristics of the patients of 3 groups classified by insight level. The only difference found in demographic variables among 3 groups according to insight level was that patients having good insight were younger than the others (p<0.01). Concerning drinking-related area, patients having fair insight had started drinking at a later age than patients having good insight (p<0.05) and patients with good insight had more prior admission experiences due to drinking problems than patients with fair insight (p<0.05). For the family environment, family adaptability of patients having good insight was higher than that of others (p<0.05) and family cohesiveness of patients having poor insight was lower than that of others (p<0.01).
Table 3 shows that the abstinence results of the subjects after discharge from the hospital are significantly correlated with their insight scores at the time of discharge. Table 4 shows the abstinence results of 117 patients. The mean (SD) IMA was 3.27 (4.36) and TMA was 4.94 (4.58). The mean IMA and TMA of 3 groups based on insight level were compared after control regarding baseline characteristics that varied across the insight levels with ANCOVA analysis using post-hoc tests (Dunnett's T3 for IMA, and LSD for TMA). Covariates in the model were age, age of first drinking, prior experiences of admission due to drinking problems, family adaptability, and family cohesiveness. After control of these variables, it was shown that the mean IMA of patients having good insight was significantly longer than that of patients having poor insight and the mean TMA of patients having good insight was significantly longer than that of others. Complete abstinence was achieved for 1 full year after discharge in 18 patients (15.4%) among 117 patients: 1 (3.2%) in poor, 10 (17.2%) in fair, and 7 (25.0%) in good insight patients. Using patients having good insight as the reference with adjustment for the differences in baseline characteristics across the insight levels, patients having poor insight showed an adjusted odds ratio (OR) of 0.07 (95% confidence interval [CI]=0.01-0.75, p<0.05) for complete abstinence for one full year after discharge and patients having fair insight had adjusted OR of 0.17 (95% CI=0.03-0.81, p<0.05).
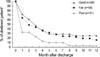
In overall comparison with 1-month stepwise life table analysis, the rate of patient continuously abstinent at each month during the follow up period was significantly different according to insight level, but the difference between fair and good insight patients was not significant in a pair-wise comparison (Fig. 1).
DISCUSSION
Generally, 15.4% of subjects remained abstinent for 1 yr. This figure is much less than 35% of other cultural area (7), but it seems to be similar with 13.1% (22) and 13.2% (23) of previous studies in Korea. Environmental difference in treating alcoholism needs to be considered in interpretation of the lower rates of abstinence. For example, Alcoholics Anonymous activities are not generalized yet to most of the Korean alcohol dependents after discharge.
The results of this study suggest that insight status, which is potentially modifiable, is a significant factor related to abstinence span in alcohol dependents. In interpretation of the results, the differences in baseline characteristics among groups based on insight level need to be considered. The patients having good insight were younger and this may have been associated with less neuropsychological damage and better cognitive flexibility. Other previous study (24) had also reported the similar finding that alcoholic patients with poor insight were more depressed and anxious. In addition, patients with good insight in this study seem to have less dysfunctional family backgrounds. Even though these covariates were corrected in this study, they may be potential factors related to the outcome.
Even though insight seems to be related to abstinence in this study, it is needed to understand its relationships with the other cognitive mechanisms that underlie alcohol dependence. It is not clear how much insight is related to other psychological factors that seem to predict better outcomes across many studies. For more clear understanding of the exact role and function of insight, additional studies are required to investigate whether insight is actually a causative factor on abstinence. Further in-depth studies are needed to know how the insight of alcoholics is related to their motivation, compliance, readiness to change and other behaviors related to recovery. Better understanding of the process of insight improvement can provide a clue to the development of effective strategies for promoting insight. Clinicians could concentrate effort on its growth if they would understand the dynamic process of insight formation (25).
The limitations of this study include the absence of sexual comparison, lack of research on additional changes in insight level and environmental situation of the subjects during the follow up period. The use of self-report information in the assessment of drinking outcomes may be another limitation of this study. Though insight state is found to be related to abstinence results after treatment, additional study is needed in other cultures and other population characteristics such as sex, specific age, ethnicity and the like.




 XML Download
XML Download