

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Etanercept is a soluble tumor necrosis factor (TNFα) receptor fusion protein, which inhibits the biological activity of TNFα. Specific therapy targeting TNFα has been offered an important advance in the treatment of active rheumatoid arthritis (RA) (1). Although anti-inflammatory and disease-modifying effect of anti-TNFα therapy are well known, there are concerns for development of serious side effects such as autoimmune disorder, infection and neoplasm as the physiologic actions of TNFα are blocked (2, 3).
Drug-induced lupus was firstly reported by Hoffman in 1945, in a patient who developed hypersensitivity syndrome similar to acute systemic lupus erythematosus (SLE) after taking sulfadiazine (4). Up to 80 kinds of drugs have been known to induce lupus-like syndrome, composing approximately 10% of the all SLE cases (5). Anti-TNFα agents including etanercept have recently been considered as drugs that can potentially induce lupus, since new autoantibodies such as antinuclear antibodies (ANAs) and anti-double stranded DNA (anti-dsDNA) antibodies were detected in anti-TNFα treated patients (6-8).
Shakoor et al. described the first SLE case among the RA patients treated with etanercept in 2002 (9). Since then, a few similar cases have been reported, that alarmed the clinicians for development of SLE in RA patients treated with anti-TNFα agents (10-13). However, all of the reported cases of anti-TNFα-induced SLE was manifested without major organ involvement and resolved shortly after the discontinuation of the therapy. Although a case of tuberculous pleurisy following infliximab therapy was reported in Korea, etanercept associated SLE was not reported previously (14). Herein, we describe a 55-yr-old Korean woman who developed overt life threatening SLE complicated by pneumonia and tuberculosis following etanercept treatment for RA.
CASE REPORT
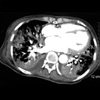
A 55-yr-old Korean woman presented with fever and generalized weakness which persisted for 3 months. She had no history of pulmonary tuberculosis or diabetes mellitus. She was diagnosed as seropositive RA 20 yr ago, and had been treated with prednisolone, NSAIDs and methotrexate. Since she had continued active joint inflammation, 25 mg of etanercept twice weekly subcutaneous injection was added to the treatment 8 months ago. Despite improvement of her arthritic symptoms, she began to experience severe fatigue and malaise 3 months ago. Intermittent high fever, myalgia, oral ulcers, gum bleeding, and 10 kg-weight loss were associated. Physical examination revealed cachexic, chronic ill looking woman with severe wasting. Her blood pressure was 130/75 mmHg, heart rate 88/min, and body temperature 38.1℃. Her hands demonstrated typical changes of RA with ulnar deviation and deformity of her fingers. Conjunctiva was anemic. Shallow irregular shaped ulcers with hemorrhagic spots were noted in the oral cavity. On chest examination, crackles were heard over both lung fields. There was no abnormal finding without hepatosplenomegaly in the abdomen. Initial complete blood count revealed hemoglobin of 7.7 g/dL, white cell count of 3,000/µL (65% neutrophil, 26% lymphocyte), and platelet of 40,000/µL. Peripheral blood smear showed no abnormal hematologic cells. Erythrocyte sedimentation rate was 11 mm/hr and C-reactive protein was positive at 0.6 mg/dL (normal <0.3). Blood chemistry values revealed a total protein of 6.6 g/dL, albumin of 2.4 g/dL, BUN 17 mg/dL, creatinine 0.6 mg/dL, AST 447 IU/L, and ALT 113 IU/L. Creatine kinase was elevated to 253 IU/L. Urinalysis revealed one positive for protein. ANA was positive at a titer of 1:640, staining speckled pattern, and rheumatoid factor was positive at 2,180 IU/mL (normal <15 IU/mL). Anti-dsDNA was positive at 14.2 IU/mL (normal <10 IU/mL). Antibodies against ribonucleoprotein and Ro/SS-A were positive, but La/SS-B and Smith were negative. C3 was 19.2 mg/dL, C4 was 9.9 mg/dL. Symmetrically narrowed joint spaces, bony erosion, and osteopenia were shown in hand radiography suggesting chronic RA with destructive change. Chest radiography revealed pneumonia and pulmonary edema in both lung field (Fig. 1). Chest CT showed pneumonia, pulmonary edema, and pleural effusion with pulmonary hemorrhage suggestive of lupus pneumonitis (Fig. 2). Bone marrow examination was normal except for increased megakaryocyte without evidence of hematologic malignancies.
A diagnosis of SLE with major organ involvement with pneumonitis and thrombocytopenia was made. Etanercept was discontinued and high dose corticosteroid was started. Lupus pneumonitis complicated with pulmonary hemorrhage was improved with corticosteroids treatment. However, residual lung infiltration remained. Bronchoscopic cell culture and PCR of sputum revealed coexistent adenoviral infection, and acyclovir was instituted. Two month later, her general condition markedly improved. However, she was complicated by unilateral pleural effusion, which showed positive for acid-fast bacilli PCR. Anti-tuberculous therapy of isoniazid, ethambutol, rifampin, and pyrazinamide was started. She is maintained on prednisolone 20 mg/day, hydroxychloroquine 300 mg/day, and nabumetone 1 g/day with minimal symptoms upon 12 months of follow up. However, she still had high titers of ANA and anti-dsDNA antibodies.
DISCUSSION
TNFα is an important pro-inflammatory cytokine that can cause inflammation and bony erosion in RA. TNFα inhibitors, such as infliximab, etanercept, and adalimumab were shown to be very effective in reducing synovial inflammation and retarding structural damage in RA patients. Anti-TNFα therapy has opened a new era in treatment of RA, and is being used more and more in current rheumatologic practice. Although TNFα inhibitors are effective therapy for RA, the concerns for serious side effects have been also raised. Adverse events that can potentially occur in anti-TNFα treated patients include tuberculosis, bacterial sepsis, heart failure, hematologic malignancy, and systemic autoimmune disease such as SLE and systemic sclerosis (15).
Autoantibody formation was reported at high frequency in anti-TNFα treated patients. In RA patients treated with infliximab, ANA developed in 29-76.7% and anti-dsDNA in 10-29% (7, 8, 16, 17). Also in etanercept treated RA patients, 11-36.3% patients had developed ANA, and 5-15% developed anti-dsDNA (16, 18, 19). In Crohn's disease, autoantibody development and infliximab-induced SLE were reported (20-24). Shakoor et al. first reported four cases of etanercept-induced SLE in a series of RA patients in 2002 (9). Swale et al. also reported a case of SLE following 12 months of etanercept therapy in the following year (10). In the previous reports, timing of the onset and offset of the SLE features strongly supported a drug related effect of etanercept. In these patients, SLE developed after mean 7.7 months (range 3-24) of commencing etanercept therapy, and were all women. Most common clinical feature of SLE was skin rash. There was no significant life threatening organ involvement such as kidney, lung, heart and central nervous system. The SLE features were resolved rapidly on stopping the treatment. The British Society for Rheumatology recommends stopping anti-TNFα therapy and appropriate treatment if symptoms of an SLE-like syndrome develop on anti-TNFα treatment (25).
The pathogenesis of anti-TNFα in development of SLE has not been yet clarified. Cairns et al. explained that TNFα may up-regulate the cellular expression of the adhesion molecule CD44, which has a role in the clearance of apoptotic neutrophil by phagocyte. Reduced CD44 expression by anti-TNFα can potentially induce SLE by abnormal clearance and exposure to apoptotic materials (12, 26). Long term exposure over 30 weeks to infliximab has been suggested as a factor that can lead to SLE in one study (17). Although autoantibody formation is quite prevalent in anti-TNFα treated patients, overt clinical syndrome of SLE is rare, suggesting development of SLE in patients treated with anti-TNFα have certain genetic or environmental factors predisposing for systemic autoimmune diseases.
As in our case, severe life-threatening SLE with major organ involvement can occur after etanercept therapy. Risk factors for development of systemic autoimmune diseases should also be evaluated before starting anti-TNFα therapy, as screening for tuberculosis recommended before anti-TNFα treatment.

 XML Download
XML Download