

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ovarian cancer is the most common cause of cancer death from gynecologic malignancy. However, it is rarely diagnosed in early stage because of the insidious growth pattern of this tumor. The management of ovarian cancer is surgery and adjuvant chemotherapy. Ovarian cancer is often initially responsive to chemotherapy but ultimately becomes refractory. There have been some efforts in molecular biology to understand chemotherapy resistance of ovarian carcinomas. In some ovarian cancers, overexpression of several genes, including HER-2/neu, myc, ras and p53 have been described (1).
The c-kit proto-oncogene encodes a tyrosine kinase receptor for stem cell factor, KIT, which is expressed in various normal and tumor tissues (2, 3). Most of the c-kit mutations have been described in gastrointestinal stromal tumors (GIST) (4). Recent studies have shown that several tumors express c-kit, such as lung (5), breast (6) and testicular (7) malignancies. Coexpression of Kit ligand and c-kit has been reported in gynecological tumors including serous adenocarcinomas and germ cell tumors of the ovary (8, 9).
However, mutational analysis of c-kit in ovarian carcinoma has rarely been published. Immunohistochemistry for the CD117 antigenic epitope identifies the KIT protein product (a tyrosine kinase receptor) of the c-kit protooncogene whose locus is present on chromosome 4q11-q12 (2). Mutations of c-kit cause constitutive activation of this receptor, which has been the target of the tyrosine kinase inhibitor, imatinib mesylate (10). The most common mutations of the c-kit protooncogene are exon 11 and exon 17 (11). Imatinib mesylate blocks signal transduction in the presence of an exon 11-activating mutation, not exon 17 (12). To determine whether treatment with imatinib mesylate might be useful in ovarian tumors, mutational analysis is essential. The purpose of our study is to determine if the ovarian epithelial carcinomas express KIT protein and to define mutational status.
MATERIALS AND METHODS
Materials
The archival materials are 43 cases of ovarian surface epithelial tumors, which are 39 patients collected from the files Pathology Department of Kyungpook National University Hospital and 4 cases from Daegu Fatima hospital from 2000 to 2004. The 43 patients are consisted of 26 cases of carcinomas, 7 cases of borderline tumors, and 10 cases of benign tumors. All the patients with carcinomas and borderline tumors underwent abdominal hysterectomy with unilateral or bilateral salpingo-oophorectomy. The hematoxylin-eosin stained slides were reviewed and one block per case representative for the tumor was selected for immunohistochemistry and mutational analysis. The clinical informations was based on the patient's medical records.
Immunohistochemical analysis
Five µm of formalin-fixed paraffin-embedded tissue sections were cut and immunostained with polyclonal rabbit antibody c-kit (A4502, Dako, Carpinteria, CA, U.S.A.). Each section was deparaffinized using xylene and subsequent hydration. The immunohistochemical studies were performed using the streptavidine-biotin-peroxidase (Ultra Vision Kit; LAB vision, Fremont, CA, U.S.A.) with diaminobenzidine (DAB) as chromogen and Mayers' hematoxylin as nuclear counterstain. The assays were performed on an automated stainer (BenchMark model; Ventana, Tucson, AZ, U.S.A.). Sections of GIST were used as positive control. The intensity of the immunostaining was graded as negative (no staining), 1+ (weak), 2+ (moderate), or 3+ (strong). Tumors staining in greater than 10% of the tumor cells were considered to be positive.
DNA isolation, polymerase chain reaction (PCR), and single-strand conformational polymorphism analysis (SSCP)
From formalin-fixed paraffin-embedded tissue samples, we cut 10-µm thick sections from each sample. Genomic DNA was extracted using QIAamp DNA mini kit (Qiagen, Germany). Exons 11 and 17 of c-kit gene were amplified by PCR using primers described in Table 1. Each PCR reaction was performed in 20 µL of reaction volume: 200 ng of genomic DNA, commercial Perkin-Elmer (PE) buffer (1×10 mM Tris-HCl, pH 8.4; 50 mM KCl), 1.5 mM MgCl2, 200 µM of each triphosphodeoxy-nucleotides (dNTP), one unit of AmpliTaq Gold (PE) polymerase, and 0.1 µM of each primers. In the case of exon 11, the reaction mixture was denatured at 94℃ for 3 min and subjected to 40 polymerization cycles (94℃ for 30 sec, 51℃ for 30 sec, and 72℃ for 60 sec). In the case of exon 17, the reaction mixture was denatured at 94℃ for 5 min and subjected to 40 polymerization cycles (94℃ for 30 sec, 51℃ for 30 sec, and 72℃ for 30 sec). PCR reaction was run in GeneAmp 9600 thermocycler (PE).
PCR-SSCP analysis for exon 11 and 17 were performed in all cases. For SSCP analysis, each PCR product was mixed with an equal volume of loading buffer (95% formamide, 0.05% bromophenol blue, and 0.05% xylene cyanol). After denaturation at 94℃ for 5 min and snap cooling on ice, 3 µL of each sample was loaded on polyacrylamide gels and subjected to electrophoresis. For the analysis of exon 11, 10% polyacrylamide gel was used and 8% gel was used for exon 17. The gels were stained using Silver Stain Plus kit (Bio-Rad, Hercules, CA, U.S.A.), according to the manufacturer's recommendation.
RESULTS
Clinical data
The 33 cases included 13 serous cystadenocarcinomas, 1 borderline serous tumor, 8 mucinous cystadenocarcinomas, 6 borderline mucinous tumors and 5 clear cell carcinomas. To compare with the benign counterparts, 5 cases of serous cystadenoma and 5 cases of mucinous cystadenoma were included in the study. The mean age was 43.3 yr (range 20 to 76 yr). The stages of the carcinomas were as follows: Stage I 11 cases, Stage II 3 cases, Stage III 12 cases. All the patients with carcinomas and borderline tumors underwent total hysterectomy with unilateral or bilateral salpingo-oophorectomy. The serous cystadenocarcinoma patients underwent omentectomy and appendectomy with careful examination of all serosal surfaces and biopsies of any suspected lesions. Ten cases of serous cystadenocarciomas had omental or pelvic metastasis of tumor cells. After surgery, a postoperative chemotherapy was performed in mucinous and serous cystadenocarcinoma, and clear cell carcinoma patients except two patients. One patient was stage Ia mucinous cystadenocarcinoma and the other was stage Ia clear cell carcinoma. The chemotherapy cycles were 6 to 12 cycles, consisted of cisplatin, cyclophosphamide and taxol. Two patients of serous cystadenocarcinoma and one patient of clear cell carcinoma recurred, but all patients are still alive.
Immunohistochemistry
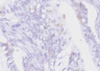
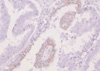
Three cases (3/6, 50%) of borderline mucinous cystic tumors and two cases (2/8, 25%) of mucinous cystadenocarcinomas showed positive cytoplasmic staining for KIT protein (Fig. 1). Only one case (1/13, 7.7%) of serous cystadenocarcinoma had positive staining (Fig. 2). The intensity was focal weak or moderate. None (0/5) of clear cell carcinomas showed positive staining. The benign mucinous and serous cystadenomas were all negative.
Mutational analysis by SSCP
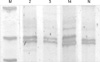
Mutational analysis was applied to all cases of carcinomas and borderline tumors. No mutation was identified at exon 11. Two cases of borderline mucinous tumors and one case of mucinous cystadenocarcinoma had mutation at exon 17 (Fig. 3, 4). In these cases, the immunohistochemistry also shows focal positive staining at epithelial component. The results are presented in Table 2.
Correlation of c-kit immunohistochemical expression and mutation with clinical parameters
In immunohistochemical results, two cases of c-kit positive mucinous cystadenocarcinoma were stage Ic and II. One case of serous cystadenocarcioma was stage IIIc with pelvic metastasis but no recurrence. In exon 17 mutational analyses, one patient with mucinous cystadenocarcinoma had stage Ic.
DISCUSSION
The evidence of surface epithelial origin in ovarian tumors is strongest for the serous, endometrioid, and clear cell subtypes and substantial for mucinous tumors (13), and greater than 95% of ovarian carcinomas originate from the surface epithelium. According to the research of Parrott et al. (14), KIT ligand and c-kit was detected in normal human ovarian surface epithelium. Their research also demonstrated that the expression of KIT ligand and receptor c-kit protein was examined at borderline tumor, stage I & stage III ovarian cancers. The intensity of immunohistochemical staining was decreased in advanced tumors. Their observations support the hypothesis that KIT ligand and c-kit may play an important role in normal ovarian surface epithelium and progression of ovarian cancer.
Based on this hypothesis, we performed c-kit immunohistochemical stain on mucinous, serous and clear cell carcinomas including borderline tumors. The study about expression of c-kit in ovarian epithelial cancers has been investigated previously, but the results vary considerably among the groups. And, most of the studies were focused on immunohistochemical expression. Little is known about c-kit mutational status and only a few studies have reported that no mutation of KIT was found in serous ovarian carcinomas (15, 16). In the research of Tonary et al. (17), there was a decrease or lack of KIT expression in advanced stage malignant ovarian tumors. As the tumor types, serous carcinomas show 76%, mucinous carcinomas 0%, endometrioid carcinomas 60%, and clear cell carcinoma 75% positive c-kit expression in immunohistochemistry. They also found that low malignant potential tumors show higher expression than malignant tumors. In contrast to this, Schmandt et al. (18) demonstrated that c-kit immunohistochemical staining was absent in low grade tumors but was present in high-grade serous carcinomas. Also, c-kit expression was correlated with progression of disease after first-line chemotherapy and chemotherapy resistance (19). Thus, there are many disparities between groups with regard to expression of KIT in ovary.
Imatinib mesylate, tyrosine kinase inhibitor has been reported to be effective in cases of tumors with an exon 11-activating KIT mutation. So, to determine the efficacy of imatinib mesylate, we performed mutational analysis on exon 11 and exon 17 of c-kit in ovarian surface epithelial carcinomas. As the result, the positive rate of c-kit immunohistochemical stain was greater in mucinous tumors than serous tumors. In mucinous tumors, borderline tumors showed higher incidence than malignant one. The c-kit immunohistochemical expression was not correlated with tumor stage or histological grade. The mutation at exon 11 was not found in any of our cases. However, mutation at exon 17 was present at two cases of borderline mucinous tumors and one case of mucinous cystadenocarcinoma with stage Ic.
The results of our study suggest that ovarian surface epithelial carcinomas show less frequent expression of KIT protein in serous type and lack KIT-activating mutation in exon 11. Although the immunohistochemistry for KIT protein show positive expression in some ovarian tumors, the therapy with imatinib mesylate may not be indicated because immunohistochemistry is not correspond to KIT-activating mutation in exon 11. It is reasonable to predict that ovarian surface epithelial tumors are unlikely to respond to imatinib mesylate and the role of c-kit protooncogene in ovarian carcinogenesis is not be clearly verified.



 XML Download
XML Download