

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dacryocystorhinostomy (DCR), which has been performed for the past hundred years, is a surgical procedure by which lacrimal flow is diverted into the nasal cavity through an artificial opening made at the level of the lacrimal sac. The operation can be carried out using either an external or endonasal surgical approach. The external approach was popularized first and became the surgery of choice for most ophthalmologists, until recently (1). Since its first description by McDonough and Meiring (2), ten years ago, endoscopic DCR has been gaining popularity, largely due to technological advances in endoscopes and other modern instruments of rhinologic surgery (3).
Despite much debate, many ophthalmologists still believe that external DCR provides a higher success rate than endoscopic DCR, and consider external DCR to be the gold standard treatment for nasolacrimal duct obstruction. Though many types of endonasal approaches have been attempted, long-term success rates have not been equivalent to that achieved with external DCR, which approximates 90% (4-7).
Endoscopic DCR with laser assistance is successful between 58 and 85 percent of the time (6,8,9), whereas endoscopic DCR procedures using other tools (eg. drill, cold knife, punch) appear to yield slightly higher success rates (10-11).
The most common cause of a surgical failure in endoscopic DCR is obstruction of the neo-ostium by granulation tissue or synechia that forms post-operatively (5-11). Most previously-described endoscopic DCR procedures involve a small opening at the medial wall of the lacrimal sac, and sacrifice nasal and lacrimal sac mucosa during the procedure. Inadequate exposure of the lacrimal sac, due to limited resection of bone and excessive and unnecessary removal or injury of surrounding nasal and lacrimal sac mucosa, and, hence, exposure of bone around a small neo-ostium, appear to contribute to obstruction of the neo-ostium by granulation tissue.
This retrospective study estimates the effectiveness of a surgical procedure that is a modification of previously reported endoscopic DCR techniques. This technique exposes the lacrimal sac fully after removing the maxillary bone surrounding the sac, creates a large marsupialized lacrimal sac, and covers the exposed bone with preserved nasal mucosal flaps.
MATERIALS AND METHODS
At our institution, from 2002 to 2004, 42 patients (3 male and 39 female) underwent 46 endoscopic DCR (17 left sides and 29 right sides) for chronic epiphora. Patients' ages ranged from 7 to 71 yr, with a mean age of 47. All patients were evaluated by an ophthalmologist before surgery. Pre-operative evaluation consisted of a standard examination that included lacrimal irrigation, conventional dacryocystography, and/or dacryoscintigraphy. The nasal cavity was examined and the need for additional nasal surgery (i.e., septoplasty, middle turbinate reduction) also was determined pre-operatively.
Of the 46 primary surgery cases, fourteen cases previously had failed insertion of a nasolacrimal polyurethane stent. Etiologies of epiphora were proximal nasolacrimal duct obstruction in all cases and one case had associated inferior canaliculi obstruction.
Patient symptoms and endoscopic findings of the neo-ostium were evaluated postoperatively. Irrigation through the punctum was performed to evaluate the patency of the neo-ostium post-operatively, and the neo-ostium was judged "wide" in size if the marsupialized sac had been well maintained in shape and size. Surgery was considered unsuccessful if the patient had one or more of the following postoperative outcomes: 1) no marked improvement of preoperative chronic epiphora, or any episode of dacryocystitis; 2) inability to irrigate the lacrimal system; and 3) nasal endoscopy revealing obstruction of the neo-ostium with granulation tissue or synechia.
Operative techniques
At our institution, DCR is performed under local or general anesthesia, as determined by considering a number of patient factors. After shrinkage of the nasal cavity by inserting a gauze packing soaked in a mixture of 1:2,000 epinephrine and 1% lidocaine, the head of the middle turbinate and the mucosa surrounding the lacrimal sac are infiltrated with a mixture of 1:200,000 epinephrine and 2% lidocaine. The patient is placed in a supine position with the head elevated 15 degrees. A zero or thirty degree, 4-mm diameter endoscope is used.
Operating steps are shown in Fig. 1. In the first step, using a slit knife (angled, 2.7 mm, Alcon Co., Cleveland, Ohio, U.S.A.), a reverse "C" shaped mucosal incision, 10×10 mm, is made at the lateral nasal wall anterior and slightly superior to the insertion of the middle turbinate (Fig. 1A). The posteriorly based mucosal flap is elevated backwards off the maxillary bone, extending up to the uncinate process. The maxillary bone covering the lacrimal sac then is gently drilled (Curved diamond DCR bur, 15 degree, 2.9 mm, Xomed Co., Jacksonville, Florida, U.S.A.) until the sac is widely exposed, extending to the level of the fundus (Fig. 1B). It is important to remove all bone covering the common cannalicular opening. Metallic lacrimal probes are passed medially through both canaliculi, and gently pushed so as to tent the sac, thus facilitating incision through the sac while precisely localizing the position of the sac lumen (Fig. 1C). An incision then is made with a slit knife, avoiding injury to the sac lumen and, hence, minimizing hemorrhage.
The elevated nasal mucosal flap is bisected and trimmed. The mucosal flaps are adjusted in size to cover the denuded bone surrounding the opened sac. The lacrimal sac flaps are incised, everted, and adjusted to accurately appose the nasal mucosa. A small gel foam patch is packed lightly in the exposed sac to keep the flap anastomosis in position throughout the initial healing period (Fig. 1D). A silicone bicanalicular tube (Canaliculus intubation set tube, Xomed Co., Jacksonville, Florida, U.S.A.) is positioned, except in those instances in which the sac is marsupialized widely due to prior longstanding dilatation of the sac.
Light nasal packing is required unless there has been associated nasal surgery (i.e. septoplasty). Post-operatively, each patient is prescribed antibiotics and ophthalmic drops, and followed regularly for nasal dressings. Irrigation and spray of the nasal cavity with saline are performed to prevent crust formation. The silicone tube generally is removed after six weeks.
RESULTS
The average follow-up period varied from three to 33 months, with an average of 5.9 months. Of 46 cases, 38 cases (83%) demonstrated primary surgical success, defined as decreased or absent epiphora and an adequately patent neo-ostium. In eight cases (17%), including one case of functional obstruction, obstruction of the neo-ostium by granulation tissue or synechia was identified, all associated with persistent epiphora (Table 1). Of 14 cases with a history of previously failed insertion of a nasolacrimal polyurethane stent, three showed obstruction (21%) while five showed obstruction (16%) out of the remaining 32 cases.
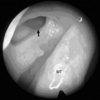
The neo-ostium was widely patent in 35 cases (76%) (Fig. 2) and "narrow but patent" in three cases (7%). Though six cases (four with wide and patent neo-ostium and two with narrow but patent neo-ostium) complained of occasional epiphora in spite of great symptom improvement postoperatively, these cases were considered surgical successes, in accordance with our prior criteria.
Among the eight patients with persistent obstruction of the neo-ostium, six subsequently underwent revision procedures. Two patients refused revision surgery and are being followed for symptoms. All six patients who underwent revision became free of epiphora and ultimately had an adequately patent ostium that has persisted throughout the mean follow-up of six months post revision surgery. Overall, 44 of 46 cases (96%) ultimately had a successful surgical outcome.
All five patients without placement of silicone tube stent after sac opening had widely patent neo-ostium without epiphora. In addition to the DCR procedure, septoplasty was performed in three cases (7%) and anterior middle turbinectomy in one case.
There were no serious complications, beyond obstruction of the neo-ostium causing surgical failure. In one case, orbital fat was mildly exposed during the operation but had no influence on the postoperative surgical outcome.
DISCUSSION
For DCR, the endoscopic approach has several advantages over the external approach: 1) it is less traumatic and, thus, shortens the hospital stay; 2) a facial scar is avoided; 3) there is no disruption of the medial canthal tendon, which consequently enables preservation of lacrimal pump function; 4) access to the sac is direct through the lacrimal bone, avoiding double-side dissection of the sac; and 5) it is excellent in controlling tissue and, thus, results in less trauma to the nasal mucosa. Conversely, disadvantages are: 1) the surgical field may be limited because of bleeding; 2) there is an occasional need for septoplasty or removal of the middle turbinate; and 3) there appears to be increased likelihood of granulation tissue formation, resulting in stenosis and, thereby, obstruction of the opening. Previously described, conventional endoscopic DCR techniques generally involved limited opening of the sac, yielding frequent obstruction of the neo-ostium by granulation tissue, an outcome which explains the higher failure rates.
To avoid or prevent obstruction of the neo-ostium, many modified techniques have been attempted. These include complete separation of the sac from the nasolacrimal duct to divert lacrimal flow to the neo-ostium (12), use of steroids or mitomycin-C (13,14), and use of mucosal flaps after wide resection of bone surrounding the sac (15-17); this last approach is technically similar to our method.
Our surgical technique modified the conventional endoscopic techniques in order to solve previously reported sources of surgical failure. Our modifications included the following: 1) A nasal mucosal flap was elevated to avoid unnecessary injury or removal of the mucosa; 2) We exposed the lacrimal sac as wide and as high as possible, up to the level of the fundus, by removing the bone surrounding the sac using a power drill; 3) Instead of cutting off the sac wall, it was incised and everted to meet the nasal mucosa; 4) Tailored mucosal flaps were created to cover all exposed bone and appose the everted lacrimal sac flap. With these techniques, we intended to make a large, epithelialized fistula, thereby potentially minimizing the formation of granulation tissue and synechia, which represent the most common causes of failure in endoscopic DCR.
Our primary success rate of 83% is similar to the rates (80-88%) reported using other endoscopic techniques performed without the use of a mucosal flap (10,11). Other investigators who have reported using techniques similar to ours have noted slightly higher primary success rates, which may not be significantly different from ours (15-17). Nonetheless, considering our original intention to reduce granulation tissue formation and synechia and, thus, increase primary success by making a large marsupialized opening, our results are somewhat contrary to our expectations. There are a few possible explanations for this. First, among our 46 patients who underwent surgery, 14 previously had failed insertion of a nasolacrimal polyurethane stent; many of these 14 had developed a constricted sac with thick walls due to chronic inflammation likely caused by long-standing placement of the stent (18). In patients with a constricted sac with thick walls, structuring a large marsupialized cavity is technically more difficult. Though statistically not significant, these patients showed a slightly increased primary failure rate compared to other patients. Second, proper postoperative care was not delivered in all of our cases, due to inadequate follow-up. Good postoperative care is a necessity and increases the likelihood of a successful outcome. With more favorable case selection and improved postoperative care, a higher success rate might have been accomplished at the time of primary surgery.
Though our primary success rate was not high enough to demonstrate advantages of our technique over others, our overall success rate after revision surgery was very high, at 96%. During revision surgery performed under local anesthesia, removal of granulation tissue or lysis of synechia which obstructed the ostium was facilitated by the previously inserted bicannalicular silicone tube exposing a wide ostium. This can be attributed to the wide opening of the sac from extensive removal of surrounding bone at the time of primary surgery. These results imply that our modified technique, though it failed to achieve a higher primary success rate compared to conventional endoscopic DCR techniques, nonetheless succeeded in achieving an excellent ultimate success rate, with technically-simpler and more highly-successful revision procedures.
The purposes of using silicone tubing are: 1) to maintain the opening of the neo-ostium; 2) to prevent or correct synechia of the canaliculus; and 3) to facilitate postoperative dressings (19,20). There are debates over the use of silicone tubing in endoscopic DCR. Some investigators have reported 81-87% success rates without using silicone tubes after endoscopic DCR, and recommend not using silicone tubing or removing it early because of granulation formation stimulated by the tubing itself (19-21). As suggested by the results of our study, in which widely-patent neo-ostium was achieved in all five cases without silicone tube stenting, a silicone tube can be used, as determined by the pre-operative status of the lacrimal sac and canaliculus.
Complications of endoscopic DCR include re-stenosis of the opening, bleeding from the nasal cavity, orbital injury, CSF leakage through a fractured ethmoid, and corneal abrasion or canaliculi erosion due to the overly-tight silicone tube placement (22). A lacrimal sump syndrome and associated recurrent infections can occur if the lower portion of the bone surrounding the sac is removed inadequately (5, 22). Our marsupialization technique opened the sac inferior to the proximal nasolacrimal duct after bone removal, thereby preventing lacrimal sump syndrome.
In conclusion, the authors obtained a large marsupialized lacrimal sac with wide removal of the covering bone and use of mucosal flaps. This technique yields a good surgical result that is comparable to the results of conventional endoscopic DCR techniques. Advantages of this procedure over the conventional endoscopic DCR techniques are two. First, primary surgical failures are amenable to technically simple and highly successful surgical revisions. Second, there is a possibility for obtaining wide ostium without silicone tube stenting.


 XML Download
XML Download