

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Until recently, the Durie Salmon (DS) staging system was primarily used in patients with multiple myeloma (MM) (1). This staging system was designed according to cell mass, utilizing hemoglobin, serum calcium, lytic bone lesions, and M component production rates as measurements, with each stage divided into A and B subgroups according to renal function.
More recently, the Southwest Oncology Group (SWOG) introduced a new staging system with beta 2-microglobulin (Sβ2M) and albumin as prognostic factors (2). The SWOG staging system has been regarded as an easy, as well as good indicator of event-free survival, first-year mortality, and long-term survival. However, the SWOG system still requires more time and practice until it becomes the standard method.
Sβ2M, which is thought to reflect known tumor cell burden, has been regarded as the most important prognostic factor in MM. Although Sβ2M concentration is influenced by kidney function, multivariate analysis showed that it remains an independent prognostic factor after correction for serum creatinine concentration (3-7).
However, in patients with mild to moderate renal insufficiency, Sβ2M may be a better indicator of glomerular filtration rate (GFR) than serum creatinine (8,9). We therefore compared Sβ2M with 24 urinary Ccr as prognostic factors in MM patients, and determined the significance of 24 hr urinary creatinine clearance (Ccr) in the staging of patients with MM.
MATERIALS AND METHODS
Subjects
We retrospectively reviewed the records of all 268 symptomatic MM patients admitted and newly diagnosed at Asan Medical Center, Seoul, Korea, from 1 January 1996 to 30 November 2003. The 24-hr urinary Ccr was available at the time of diagnosis for 170 of these symptomatic MM patients, and these 170 patients were enrolled into the study. Survival time was followed until 30 April 2005.
All the patients had symptomatic MM in accordance with the diagnostic criteria of the International Myeloma Working Group (2003) (11). These criteria are defined as: 1) M-protein in serum and/or urine; 2) bone marrow (clonal) plasma cells or plasmacytomas; 3) related organ or tissue impairment (end organ damage, including bone lesions); and 4) no minimal level of clonal bone marrow plasma cells.
Patients with nonsecretory myeloma, smoldering multiple myeloma, POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes), plasma cell leukemia, light chain deposit disease, MGUS (monoclonal gammopathy of undermined significance), extramedullary plasmacytoma, a combination of other malignancies, severe trauma were excluded.
Parameters
We investigated age, sex, heavy chain types, light chain types, Durie-Salmon stage, Sβ2M, hemoglobin, serum calcium, serum albumin, serum creatinine, and 24 hr urine creatinine clearance before chemotherapy. Sβ2M was measured by a radioimmunoassay with125I-labeled beta 2-microglobulin.
Treatment
Whereas patients received various treatments, they could be divided into 3 groups; those who received conservative treatment (no treatment or dexamethasone [20 mg/m2orally] only), those who received conventional chemotherapy (e.g., VAD, MP, high dose cytoxan plus predinisolone, and thalidomide plus dexamethasone regimens), and those who received autologous stem cell transplantation.
The MP regimen consisted of melphalan (8 mg/m2) and prednisolone (60 mg/m2) for 4 days; the VAD regimen consisted of vincristine (0.4 mg), doxorubicin (9 mg/m2) for 4 days, and dexamethasone (40 mg) for 12 days. The high dose cytoxan plus prednisolone regimen consisted of cytoxan (400 mg/m2) for 1 day and prednisolone (40 mg/m2) for 7 days and was a variant of the VBMCP (vincristine, BCNU, melphalan, cytoxan, prednisolone) regimen. The thalidomide plus dexamethasone regimen consisted of 200 mg thalidomide orally per day plus 5 to 10 mg dexamethasone intravenously 4 times per day.
Survival time
Medical records were used to collect data. Interviews with patients' families by telephone and data from the hospital network connected to the Korean National Statistical Office were also utilized to determine the patient survival times.
Staging system
Patients were divided depending on DS stage, which was assigned by physicians who first examined them (1). Then, they were resorted by SWOG staging system according to Sβ2M and albumin concentrations (2).
SWOG stage 1 was defined as Sβ2M <2.5 mg/L; stage 2 as 2.5 mg/L ≤Sβ2M <5.5 mg/L; stage 3, Sβ2M ≥5.5 mg/L and serum albumin ≥3.0 g/dL; and stage 4, Sβ2M ≥5.5 mg/L and albumin <3.0 g/dL.
During the course of this study, we formulated a new experimental staging system based on 24 hr urinary Ccr and serum albumin. In this system, stage 1 defined as Ccr ≥90 mL/min; stage 2 as 90 mL/min >Ccr ≥30 mL/min; stage 3 as Ccr <30 mL/min and albumin ≥3.0 g/dL; stage 4 as Ccr <30 mL/min and albumin <3.0 g/dL.
Statistical analysis
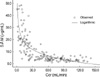
SPSS (version 11.0) was used to determine the means and standard deviations and medians of patient characteristics of patients and laboratory findings. One-way ANOVA and Student's t test were used to compare mean Ccr according to heavy or light chain types. An interactive graph of Ccr and Sβ2M was drawn using a scatter plot and a logarithmic estimated curve.
The Kaplan-Meier method was utilized for survival analysis with log rank test; statistical significance was defined as p value less than 0.05.
The Cox proportional hazard model was employed for univariate analysis and multivariate analyses to confirm the significance of risk factors of death. In multivariate analysis, we used eliminated variables stepwise (backward) by a significance of less than 10%.
RESULTS
Study population
From 1 January 1996, through 30 November 2003, 289 patients with plasma cell disorders were admitted to our Center. Among them, there were 268 symptomatic MM patients. We excluded 14 patients with other monoclonal gammopathies and 7 patients with combining other malignancy or severe trauma. Gammopathies other than symptomatic multiple myeloma were 3 MUGS, 2 plasma cell leukemia, 2 smoldering MM, 2 nonsecretory MM, 1 extramedullary plasmacytoma, 1 multiple solitary plasmacytoma, and 3 POEMS. As to 170 patients, 24-hr urinary creatinine clearance was available at the time of diagnosis. Baseline characteristics and laboratory findings at the time of diagnosis are shown in Table 1.
Table 2 shows the mean Ccr of each type. The mean Ccr in patients with free light chain was lower than those of the heavy and light chain type groups. Mean Ccr of patients with free light chain was 36.2 mL/min, whereas those of patients with IgG type and IgA were 54.9 mL/min and 62.2 mL/min (p=0.005), respectively. However, mean Sβ2M of patients according to heavy chain types was not significantly different(p=0.156).
Of the 170 patients, 28 patients were managed conservatively, 92 patients were treated with conventional chemotherapy, and 50 patients received high-dose chemotherapy with autologous stem cell transplantations. The first-line chemotherapy regimens consisted of VAD in 94 patients, MP in 41, cytoxan plus prednisolone in 4, thalidomide plus dexamethasone in 1. The chemotherapy regimen was unidentified in 2 patients.
We could definitively identify cause of death only if patients died in hospital, although we attempted to interview by telephone family members of patients who died outside of hospital to exclude death by accidental trauma. Of the 51 patients who died in hospital, 28 died of sepsis, 9 of respiratory failure, 4 of heart failure, 2 of major bleeding, 1 of arrhythmia, 3 of acute renal failure, 1 of acute myocardial infarction, 1 of subdural hemorrhage, and 2 of hepatic failure.
Among the 268 symptomatic MM patients, only 3 patients had hemodialysis before diagnosis because of acute renal failure; these patients did not have any other specific etiology, such as diabetes mellitus or hypertension. In all 3 persons, Ccr was measured at diagnosis, and all 3 were enrolled in this study.
Univariate and multivariate analysis
Univariate analysis showed that age, serum calcium, serum creatinine, Sβ2M, Ccr, free light chain type, and treatment modalities were significant prognostic factors, using both the continuous and dichotomous methods (Table 3). The conservative management group had a shorter life expectancy than both the conventional chemotherapy group (hazard ratio [HR] 2.021, p=0.004) and the autologous transplantation group (HR 9.020, p<0.001). However, Sβ2M concentration was not significant in univariate analysis of 104 patients with Ccr ≥30 mL/min (HR 1.001, p=0.982) (Table 4).
Multivariate analysis of prognostic factors using the Cox proportional hazard model showed that serum Sβ2M, creatinine clearance, and treatment modalities were significant prognostic factors in continuous method (Table 6). Ccr was of borderline significance and was not eliminated by backward stepwise calculation if p=0.10. Using the dichotomous method, however, the result was somewhat different. If the Ccr cut-off value was 30 mL/min and that of Sβ2M was 5.5 mg/L, Ccr and treatment were significant, but Sβ2M concentration was not. This discrepancy was due to the close relationship of Sβ2M and Ccr, making it difficult to determine a standard cutoff value using the dichotomous method.
Correlation of beta 2-microglobulin and creatinine clearance
When we drew a scatter plot of Sβ2M and Ccr prior to the start of chemotherapy (Fig. 1), we found that pretreatment Sβ2M was inversely related to Ccr (Spearman's correlation efficient -0.787, p<0.001).
Stage
Fig. 2 shows survival curves relative to DS stage and SWOG stage. Because we enrolled only patients whose DS stage was recorded by doctors at the time of diagnosis, the total number according to DS stage was 147 (95 dead, 52 alive). Because Sβ2M was not checked in 3 patients in the study group, the total number according to SWOG stage was 167 (112 dead, 55 alive).
Median overall survival times according to DS stage were 919 days for stage 1 (n=11), 1011 days for stage 2 (n=17), 925 days for stage 3A (n=66), and 380 days for stage 3B (n=53).
Median survival times according to SWOG stage were 1475 days for stage 1 (n=18), 917 days for stage 2 (n=65), 453 days for stage 3 (n=57), and 152 days for stage 4 (n=27) (log rank test <0.0001).
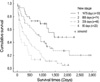
Possible staging system
Univariate analysis showed that, as Ccr increased, patient survival time increased. Furthermore Sβ2M was closely related with Ccr. We therefore formulated a new staging system based on Ccr instead of Sβ2M, plus serum albumin (Fig. 3). According to this system, stage 1 is Ccr ≥90 mL/min; stage 2 is 90 mL/min > Ccr ≥30 mL/min; stage 3 is Ccr <30 mL/ min and albumin ≥3.0 g/dL; stage 4, Ccr <30 mL/min and albumin <3.0 g/dL.
Applying this system, we found that 30 patients (12 dead, 18 alive) were stage 1, 74 (44 dead, 30 alive) were stage 2, 46 (42 dead, 4 alive) were stage 3, and 20 (17 dead, 3 alive) were stage 4.
According to this staging system, the median survival times were 1,475 days for stage 1, 889 days for stage 2, 339 days for stage 3, and 95 days for stage 4 (log rank test <0.0001).
DISCUSSION
In MM, the importance of Sβ2M has led to the introduction of the SWOG staging system. In an attempt to determine the relationship between Sβ2M and kidney function and to choose a more significant prognostic factor, we were unable to find any study that included both 24 hr urinary Ccr and Sβ2M as prognostic factors. Thus, to our knowledge, this study is the first to include both of these as prognostic factors.
We found that in MM, Sβ2M and Ccr were more closely related than we expected. Multivariate analysis showed that Sβ2M, Ccr, and treatment modalities were independent prognostic factors. Thus, the results of this study suggest that Ccr is a new, powerful prognostic factor in the patients with MM. Moreover, this finding indicates that Ccr can be incorporated into a discrete new staging system for MM.
It was interesting that Sβ2M was not significant in patients whose Ccr was greater than 30 mL/min. That is, the incremental addition of Sβ2M concentration was not a significant prognostic factor if kidney function was relatively good. Thus, the effect of Sβ2M on patient survival might be mainly due to declining kidney function.
Our new staging system used Ccr instead of Sβ2M. The latter is not likely to be a specific tumor marker in MM. This finding indicates that patient survival is related to the decreased excretion of Sβ2M rather than to its overproduction. There is evidence that Sβ2M reflects glomerular filtration rate in many situations, although it also reflects tumor cell mass (9-11). Although our Kaplan-Meier curves of stages relative to Ccr and serum albumin concentrations were discrete, they were unable to show that Ccr was a more significant prognostic factor than Sβ2M. These two factors, plus serum creatinine, are related, and other conflicting factors affect survival, thus making interpretation difficult. Differences in mean Ccr between patients with both heavy and light chains and those with only free light chains may be related to different survival times. Although the SWOG staging system has been regarded as easier and likely to supersede the DS staging system, it is cautious to determine the superiority between the two staging systems. Serum albumin was not a significant prognostic in univariate analysis, but, in the SWOG staging system, it was important in sorting patients with advanced stage MM.
Our study had several limitations. First, we may have included patients who died accidentally, since the causes of death of patients who died outside the hospital could not be determined. Second, this retrospective study did not include important parameters such as performance status, C reactive protein, chromosome 13 abnormality, and plasma cell labeling index (12,13).
In conclusion, we found that in patients with MM, Sβ2M was an independent significant prognostic factor in multivariate analysis that included Ccr. Although closely related to Sβ2M, Ccr was also a significant prognostic factor that could replace Sβ2M in staging systems of MM. Mean Ccr differed among heavy chain types, and these differences were likely related to different survival times.






 XML Download
XML Download