

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatitis B virus (HBV) infection is highly prevalent in Africa and Asia, and in the different countries, the infection rate ranges from 5% to 20%. In Korea, its prevalence has been decreasing since the HBV vaccination was introduced about 20 yr ago. Nevertheless, HBV infection still ranges from 2 to 8.9% (2-12), which is higher than in the United States and Western Europe (1). Health care workers (HCWs) in Korea are at risk for getting an infection with HBV; therefore, HBV vaccination has been strongly recommended for them. However, studies on the HBV markers for HCWs in Korea are rare. This study was initiated to determine the seroprevalence of HBsAg, anti-HBs and anti-HBc in HCWs in Korea. This study was approved by the institutional review board at our hospital.
MATERIALS AND METHODS
Surveillance of HBV vaccination history
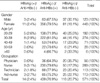
The study was performed at Sanggye Paik Hospital, which is a 700-bed university-affiliated tertiary hospital located in the northeast section of Seoul. Of the 725 HCWs working at the hospital in December, 2003, 571 of them participated in a cross-sectional HBV viral marker study and they replied to the surveillance questionnaires we gave them about their previous HBV vaccinations. The participant distributions according to age, sex and occupations are listed in Table 1. Of the 571 HCWs (123 males and 448 females), 289 (50.6%) were nurses and 466 (81.6%) were under 40 yr of age. The compliance rates according to the occupation were 33.7% (56/166) for physicians, 99.7% (289/290) for nurses, 79.6% (113/142) for aid-nurses and 89.0% (113/127) for technicians; the total compliance rate was 78.8%. Anyone inoculated at least once was classified as the vaccinated group: according to the number of doses, they were divided into the complete (3 or more) and incomplete (1 or 2) vaccinated groups.
Study on HBsAg, anti-HBs and anti-HBc, IgG
A total of 571 samples were tested for HBsAg and anti-HBs with using electrochemiluminescence immunoassay (Elecsys 2010, Roche, Mannheim, German). Samples with a cutoff index greater than or equal to 1.0 were considered positive for HBsAg, and 10 mIU/mL was set as the minimal protective level (positive) of anti-HBs. For the tests for anti-HBc with using a chemiluminescence enzyme immunoassay (ADVIA, Centaur, Bayer, Tarry town, NY, U.S.A.), the specimens with index values greater than 1.0 were considered positive.
All statistical analysis was done using SPSS for Window software, version 11.5.
RESULTS
Participant distributions according to HBsAg and anti-HBs
The overall positive rates of HBsAg and anti-HBs were 2.4% (14/571) and 76.9% (439/571), respectively (Table 2, 3). A number of HBsAg and anti-HBs co-negative cases were 118 (20.7%). The positive rates of HBsAg among the male and female groups were the same (2.4%); however, the positive rate of anti-HBs was higher in the females (79.5%) than in the males (67.5%) (odds ratio: 0.43, p value: 0.003 by chi-square test). According to occupations, the positive rate of HBsAg was the highest in the nurse group (3.1%). The positive rate of anti-HBs was the highest in the nurse group (79.6 %) and the lowest in the physician group (64.3%). The odds ratios for the nurses, technicians and aid-nurses were slightly elevated, but this was statistically insignificant. According to age, the positive rates of both HBsAg and anti-HBs were the highest for the HCW in their thirties, and the positive rate of anti-HBs was the lowest for the HCW in their sixties (odds ratio: 1.04, p value: 0.01).
Anti-HBs titers according to age, gender and occupation
Among the 439 anti-HBs positive cases, 321 cases (73.1%) had greater than a 100 mIU/mL level of anti-HBs (Table 4). The anti-HBs titers from 100 mIU/mL to <1,000 mIU/mL had the same prevalence among all the age groups (except those workers older than 60) and all the occupational groups. The anti-HBs titers from 10 mIU/mL to <100 mIU/mL were prevalent in HCW in their sixties. The anti-HBs titers greater than 1,000 mIU/mL were prevalent in the physician and nurse groups, compared with the aid-nurse and technician groups (25% and 23.2% vs. 17.7% and 12.4%, respectively).
HBsAg, anti-HBs, anti-HBc and HBV vaccination history
Of the 571 cases, only 151 cases (26.4%) showed anti-HBc positivity and 78.1% (118/151) of them were positive for anti-HBs (Table 5). Among the 420 anti-HBc negative cases, 321 cases (76.4%) were positive for anti-HBs. Therefore, in the 439 anti-HBs positive cases, the rate of infection-induced (anti-HBc positive) anti-HBs was 26.9% and the rate of vaccine-induced (anti-HBc negative) anti-HBs was 73.1%. The number of vaccine doses and the anti-HBs positive rates were significantly associated in the anti-HBc negative group (p=0.01, chi-square test). Any HBsAg positive case was not observed in the anti-HBc negative group, in contrast to the 9.3% HBsAg positive rate (14/151) in the anti-HBc positive group. In the HBsAg (-)/anti-HBs (+)/anti-HBc (-) group, there were 50 cases noted that had no vaccination history. In the anti-HBs (+)/anti-HBc (+) group, 41 cases had a history of more than 3 vaccine doses, and 4 of them even showed to be positive for HBsAg.
DISCUSSION
The prevalence rate of HBsAg in Korea is known to be about 2-8.9%, and this rate has decreased in the past 20 yr since HBV vaccination was introduced (2-12). The positive rate for HBsAg in our study is 2.4%. A study carried out in 2003 revealed that the prevalence rates of HBsAg in Korea showed a decreasing tendency from 1.9% in adults to 0.2-0.3% in elementary school children (5). Therefore, the positive rate in our study showed results similar to the study done in 2003. Several studies have been performed in the moderate HBV-endemic areas, and they reported the HBV prevalence in HCWs as ranging from 2.8% to 9.7% (13-15). The overall anti-HBs positive rate in the present study was 76.9%, and it was similar to the anti-HBs positive rate in the general Korean population (2-4, 7).
The compliance rate of our surveillance was 78.8%. However, it varied according to the occupation (33.7-99.7%) and it was lowest in the physicians group (33.7%). The main reason for this might be that the physicians were 'too busy to participate in a study' as was observed in another study (16). The physician group showed the lowest anti-HBs positive rate among the occupational groups. Possibly the higher HBsAg (-)/anti-HBs (-) rate was due to the relatively older age distribution than was seen for the other groups. In the physician group, 48.2% were older than 40 yr of age and only 63% of them was anti-HBs positive, which was below the overall anti-HBs rate. The positive rates of HBsAg and anti-HBs in the nurse group were the highest among the occupational groups. This suggested that the nurse group has more chances to be exposed to the needle stick injury or other infectious body fluid from patients than did the other occupational groups (17, 18), because most of these exposures occur during the disposal of used syringes and recapping (19). Subjects with anti-HBs levels above 100 mIU/mL were regarded as good responders and this titer was usually followed by long-term immunity (20-23). Persistence of anti-HBs is known to be related to the maximum antibody level (20, 21). Although our study was a cross-sectional study and the anti-HBs titers were not at the peak level after a basic course of vaccination, the subjects with a titer higher than 100 mIU/mL anti-HBs seem to be meaningful. This is because the subjects that develop higher anti-HBs titers will retain antibody for a longer period than those subjects with lower levels of antibody. It has been reported that once a level above 10 mIU/mL anti-HBs is acquired, it is unnecessary to give a booster dose even when the anti-HBs level falls below 10 mIU/mL (24).
We must consider the distribution of anti-HBs in relation to the anti-HBc and the vaccination history. Anti-HBc is a remarkable marker to differentiate vaccine-induced anti-HBs from infection-induced anti-HBs. Although no difference was found between the anti-HBc positive and negative groups for the anti-HBs positive rates, the anti-HBs in our HCWs were mainly acquired from vaccination (73.1%). In our study, the positive rate of anti-HBc was 26.4% (151/571) and the rate of the anti-HBc-alone positive cases was 3.3%. The positive rates of anti-HBc in the all the study cases/anti-HBc-alone in Korea have been variably reported; 55.8/19% in 1985 (2), 24.9/1.9% in 1997 (3) and 57.2/5.1% in 2000 (4). The subjects of the studies done in 1985 and 2000 were mainly adults who were aged more than 40 yr old. However, those subjects in the 1997 study and in our study included more of the younger generation Koreans who were in their twenties and thirties. A study done in 1994 (25) showed similar anti-HBs positive rates between the vaccinated and non-vaccinated groups, but another study done in 2000 revealed a higher anti-HBs positive rate in the vaccinated group in Korea (4). A study done in the South Africa revealed that the anti-HBs positive rate in HCWs was 36.6% and only 21.2% of them had a history of past immunization against HBV (26). The anti-HBs seropositivity in Turkish HCWs was reported as 68.4% (13). The seroprevalence of anti-HBc was reported as 32% in Yemen HCWs (27). Therefore, the seroprevalence rates of HBsAg and anti-HBs in Korean HCWs were similar with the prevalence rates in the general Korean population, but the Korean HCWs had lower HBsAg rates and higher anti-HB rates than did the HCWs in the HBV endemic Korea.
Out of 571 cases, 532 cases replied to the questionnaires about HBV vaccination and 74.1% (394/532) of them had previous vaccination histories (206 complete and 188 incomplete). However, 19.8% (78/394) of the vaccinated cases were anti-HBc positive and incomplete vaccination might be one of the reasons for this. Some Korean adults might have taken a HBV vaccination dose during a latent period or a window period after their HBV infections. They even had a vaccination dose after the acquisition of infection-induced anti-HBs with or without a HBV viral maker study for the booster doses. The 50 cases showing HBsAg (-)/anti-HBs (+)/anti-HBc (-)/vaccination (-) results could not be explained well. Incorrect memories or unreliable answers to the surveillance questionnaires about their vaccinations could be the reason. The vaccination done in childhood could be a reason for their incorrect memories. Such results were also observed in other study, in which 10.2% of HBsAg (-)/anti-HBs (+)/anti-HBc (-) cases had no previous vaccination histories (4).
In conclusion, 76.9% of HCWs in a Korean hospital were positive for anti-HBs and 73.1% of them had an anti-HBs level of more than 100 mIU/mL, which suggests long lasting immunity. About 25% of HCWs may need vaccination against HBV infection in case of HBV exposure, such as could happen with a needle stick injury (28).




 XML Download
XML Download