

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary tumors of the heart are rare, occurring at a frequency of 0.02% in pooled autopsy series. Secondary or metastatic cardiac tumors occur more frequently, with an at least 100 times higher, than primary cardiac tumors. Although every malignant tumor can metastasize to the heart, the common tumors with cardiac metastatsis are carcinomas of the lung, the breast, and the esophagus, malignant lymphoma, leukemia, and malignant melanoma (1).
Adrenocortical carcinoma (ACC) is a rare malignant neoplasm with poor prognosis and it occurs approximately 0.5-2 out of 1 million population per year. It grows rapidly and 82% of the patients already had dissemination of the tumor. Usual metastatic sites are the lung (71%), lymph node (68%), liver (42%), and bone (26%) (2-4). However, intracaval invasion extending into the right atrium is very rare and only several cases were reported (5-14).
Spontaneous regression of tumor is an interesting phenomenon and well documented in some types of tumor, but occurs infrequently. Although spontaneous regression of cancer has been reported in almost every type of cancer, the largest numbers of cases are reported in a few types of cancer such as neuroblastoma, renal cell carcinoma, and leukemias/lymphomas (15-18).
We report a case of non-functioning huge ACC extending into the inferior vena cava and right atrium in a young man which showed a tendency of spontaneous regression.
CASE REPORT
A 34-yr-old male patient presented with progressive dyspnea, weight loss, and poor oral intake over 3 months. Physical examination revealed increased jugular venous pulsation and decreased breathing sounds on right lower lung fields, and palpable 10 cm sized non-tender mass on right upper quadrant of abdomen.
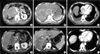
Laboratory findings revealed no significant abnormal findings except for mild leukocytosis (12,000/µL). Chest radiograph revealed moderate amounts of right pleural effusion. Abdominal sonography revealed a huge lobulated mass in right adrenal gland. Abdominal and chest computed tomography (CT) revealed 17×10 cm sized huge lobulated mass arising from right adrenal gland, tumor thrombi in the inferior vena cava (IVC), and right atrium (RA) (Fig. 1). Transthoracic echocardiography (TTE) revealed large right atrial mass which occupied nearly entire space of RA. On subcostal view, the RA mass connected continuously into IVC (Fig. 2).
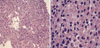
Hormonal study of adrenal gland was normal. Gun biopsy of the mass revealed cellular pleomorphism with large nuclei, abundant cytoplasm, and numerous small vascular channels which was compatible findings of endocrine tumor (Fig. 3). After pathological diagnosis of non-functioning ACC, 5-fluorouracil, adriamycin, and carboplatin based chemotherapy and radiotherapy were done. However, tumor burden was not changed and toxic hepatitis and thrombocytopenia were developed. Platelet count was lowered to 15,000/µL. Liver enzymes and bilirubin were elevated. Bone marrow biopsy revealed increased number of megakaryocytes without abnormal cells suggesting immune thrombocytopenic purpura (Fig. 4). Steroid therapy was started. Platelet count was normalized 1 month later from the initiation of steroid therapy and liver function tests were also normalized. His subjective symptoms and general conditions were improved and the patient was discharged.
During out-patient clinic follow-up, abdominal CT and TTE, rechecked 3 months after discharge, revealed marked reduction of adrenal and RA tumor burden (Fig. 1, 2). Surgical removal of primary tumor including carvoatrial mass using cardiopulmonary by-pass is recommended, but the patient refused surgery. Thus, we manage the patient conservatively in out-patient clinic. The patient showed good general health status and had no subjective symptoms during 8-month clinical follow-up.
DISCUSSION
Metastases to the heart are much more common than primary cardiac tumors. Metastatic tumors may reach the heart usually via lymphatic or hematogenous route, or by direct invasion. Transvenous extension of tumors along the IVC into the right atrium, however, is a rare condition. Some types of tumors such as hepatocellular carcinoma, renal cell carcinoma, or leiomyoma of the uterus can metastasize in such fashion (1). ACC is a rare malignant neoplasm and usually metastasize to the lung, lymph node, liver, and bone. ACC may also extend to adjacent vasculatures such as renal veins and IVC, usually accompanied by a thrombus (2-4). However, intracaval invasion extending into the right atrium is very rare and several cases were reported (5-14). Including the case of Rosen et al. (14), most of the described cases of ACC extending to RA were originated from right adrenal gland and also had tumor thrombi in IVC. This finding suggest that ACC invade directly to IVC and RA. Hedican and Marshall reported 3 cases and reviewed 26 previously reported cases of ACC (11). According to their report, about half of cases showed direct invasion of IVC and RA. As described above, our case also revealed direct invasion of right ACC to IVC and RA. To the best of our knowledge, this is the first case of ACC with direct invasion of the IVC and RA in Korea.
Approximately 60% of ACC cases presents with symptoms and signs of adrenal steroid hormone excess. However, the hormonal study was normal in our patient. Patients with a nonfunctioning ACC, just as our case, usually present with symptoms related to local mass effect like abdominal fullness, pain, indigestion, poor oral intake, nausea and vomiting.
Because chemotherapy has limited value in the treatment of ACC, complete surgical resection is the treatment of choice (1,23). Our patient had advanced ACC with IVC and RA invasion. Several reports suggested that complete surgical removal of primary tumor with carvoatrial mass using cardiopulmonary bypass is the treatment of choice (6-8,12,14). However, our patient refused surgery. In patients with advanced local or metastatic disease, not amenable to surgical resection, cytotoxic chemotherapy may be attempted. Several cytotoxic agents has been used as single drug or in combination to treat advanced ACC including cisplatin, doxorubicin, etoposide, vincristine, and 5-fluorouracil (FU) (1,23). Our patient received chemotherapy using 5-FU, adriamycin, and carboplatin, but tumor size were not changed but toxic hepatitis and thrombocytopenia developed. Thus, the patient was managed conservatively.
Spontaneous regression of tumor is an interesting phenomenon and well documented in some types of tumor, but occurs infrequently. Spontaneous regression of neoplasms occurs when the malignant tumor mass partially or completely disappears without any treatment or as a result of a therapy considered inadequate to influence systemic neoplastic disease. Although spontaneous regression of cancer has been reported in almost every type of cancer, the largest number of cases are reported in a few types of cancer such as neuroblastoma, renal cell carcinoma, and leukemias/lymphomas (15-17). In Korea, Seo et al. reported a case of spontaneous regression of liver metastasis in stage IV-S neuroblastoma after adrenalectomy (18). However, spontaneous regression in the case of ACC is very rare (19-22). Saracco et al. reported a case of spontaneously regressing ACC in a newborn (19). Kasat et al. reported a case of cortisol-producing ACC in an infant which showed complete spontaneous regression (22). In our case, the patient received chemo-radiotherapy, but the size of tumor was not changed for at least 3 months. Three months after the discharge, however, the size of adrenal mass as well as RA mass showed marked reduction despite of conservative management. The exact mechanism of spontaneous tumor regression is not established, but immunemediated process, hormonal factors, inhibition of tumor growth by growth factors or cytokines, elimination of carcinogens, angiogenesis, tumor necrosis, apoptosis, or genetic factors would be involved (15-16).
In summary, we report a case of 34-yr-old male patient who had non-functioning huge adrenal carcinoma extending into inferior vena cava and right atrium. This tumor showed spontaneous regression.


 XML Download
XML Download