

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In 1945, atomic bombs were detonated over Hiroshima and Nagasaki, Japan, toward the end of World War II. These bombs resulted in an estimated 140,000±10,000 casualties in Hiroshima and 70,000±10,000 in Nagasaki (1). At that time, Korea was occupied by Japan, and the Japanese Imperial Government had drafted numerous Koreans as soldiers and workers in munitions factories in Japan. Koreans also moved to Japan to earn a living. Thus, the atomic bombs dropped on Hiroshima and Nagasaki killed or injured numerous Koreans along with Japanese. Ichiba Junko has estimated that 30,000 Koreans died and 20,000 survived at Hiroshima and that 10,000 died and 10,000 survived at Nagasaki. Of the 30,000 total Korean survivors, about 23,000 returned to Korea, and 7,000 stayed in Japan (2). Hard times for the survivors did not end after their return. They not only suffered from poor health but also experienced hardships such as the Korean War and poverty. Many of the survivors have since died, while others are reluctant to reveal that they are, in fact, survivors owing to concerns about social prejudice. The Korean atomic bomb survivors were not recognized by the Japanese government until the 1990s and only then as the result of prolonged efforts by the survivors. In 2004, 2,235 Koreans were registered as atomic bomb survivors in Republic of Korea(3).
The association between atomic bomb exposure and malignant diseases is well established (4-6). In addition, recent studies have demonstrated that atomic bomb exposure also affects non-cancer diseases, such as myocardial infarction, thyroid disease, and chronic liver disease (7,8).
While many studies have examined the health of Japanese atomic bomb survivors, no previous study has been conducted on the health of Korean A-bomb survivors. The objectives of this study were to examine non-cancer diseases of Korean A-bomb survivors who were in residence at Hapcheon and to evaluate whether this prevalence was significantly higher than that in people not exposed to the A-bomb.
MATERIALS AND METHODS
Study population and health examination
Health examinations were conducted in 2004 at Hapcheon, Republic of Korea, because a large number of Korean A-bomb survivors currently reside at Hapcheon. A total of 223 Korean A-bomb survivors, 10.0% of all the Korean A-bomb survivors alive in the Republic of Korea in 2004, participated in the health examination. Individual atomic bomb exposure histories of Korean A-bomb survivors who participated in the health examination and lived at Hapchoen were collected using a self-administered questionnaire. Physicians and medical students interviewed the survivors to confirm the validity of their statements. Reference was also made to the atomic bomb survivor registry cards issued by the Japanese government.
The controls in this study were recruited from participants in the second Korea National Health and Nutrition Examination Survey (K-NHANES). The K-NHANES surveys a random sample of the general Korean population to assess the health and nutrition status of the population through interviews and health examinations (9). Of the total 37,769 Koreans who provided information about their health and nutrition in the second K-NHANES, 6,786 participated in a health examination, and 1,233 of these were of the same age as the participants in the 2004 Korean atomic bomb survivors'health examination in Hapcheon. Given that Hapcheon is a rural area, we selected residents of rural areas (n=463) from among the 1,233 candidates, to exclude the socioeconomic effect of residency. As the proportion of female controls was higher than that of survivors, we randomly eliminated 91 females to balance the sex ratio between the two groups. In the end, 372 persons were selected as controls.
The clinical indicators of non-cancer diseases evaluated in this study were anthropometric measurements (height and weight), systolic and diastolic blood pressures, blood chemistry (aspartate aminotransferase, alanine aminotransferase, fasting glucose, total cholesterol, blood urea nitrogen, and creatinine), hepatitis B surface antigen, and urinalysis (urine glucose, protein, and occult blood).
A participant with high systolic (≥140 mm Hg) or diastolic blood pressure (≥90 mm Hg) was classified as having hypertension, in line with the guidelines of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (10). A participant taking antihypertensive medications was also classified as having hypertension. Individuals with a serum aspartate aminotransferase (AST) or alanine aminotransferase (ALT) level higher than 0.58 µkat/L (>35 IU/L) were considered to have chronic liver disease. Those with a fasting glucose value higher than 6.1 mM/L (>110 mg/dL) and those undergoing medical treatment for diabetes mellitus (DM) or impaired glucose tolerance (IGT) were considered to have DM+IGT. Individuals with a total serum cholesterol level of 6.2 mM/L or higher (≥240 mg/dL) were considered to have hypercholesterolemia. Participants with a serum blood urea nitrogen (BUN) level higher than 7.1 mM/L (>20 mg/dL) or creatinine higher than 106 µM/L (>1.2 mg/dL) were considered to have renal function abnormality. The National Human Rights Commission of Korea approved the study protocol, and all the survivors Korea approved the study protocol, and all the survivors who participated in the health examination gave their informed consent.
Statistical analysis
The univariate analysis between the survivors and controls used Student's t-test and the Wilcoxon rank-sum test for continuous variables or the chi-square test for discrete variables.
Crude and adjusted prevalence ratios (PRs) of non-cancer diseases were obtained using both PROC PHREG and PROC GENMOD with binomial distribution and log link function in SAS version 9.0 (11). Age, body mass index, gender (male/female), marital status (married/unmarried, separated, bereaved, and divorced), education (at least a high school education/educated below high school level), usual alcohol consumption (drinks at least 1-2 times per week/drinks fewer than 1-2 times per week), and smoking status (non-smoker/ex-smoker/current smoker) were included as covariates for obtaining adjusted PRs.
RESULTS
Nearly all (96.9%) survivors were residing in Hiroshima when the bomb was dropped. The majority of the participants were exposed to the atomic bomb during their childhood or adolescence: 1.3% were in utero, 57.8% were less than 10 yr old, and 31.4% were between 10 and 19 yr at the time of the bombing. We identified the distances from the hypocenter for 122 (54.7%) survivors at the time of the bombing, based on the A-bomb survivor registry cards issued by the Japanese government: 21 (9.4%) were within 1.5 km, 55 (24.7%) were between 1.5 and 2.5 km, and 46 (20.6%) were beyond 2.5 km from the hypocenter. Unfortunately, we were unable to identify the distances for 101 (45.3%) survivors. Of the survivors, 57.0% responded that they were indoors (43.5% in wooden building, 3.6% in concrete building, and 9.9% in other structures such as shelters, trains, or unidentified buildings), 27.8% responded that they were outdoors (16.1% were in the shade of buildings or trees and 8.1% were unsheltered), and 18.8% were unable to recall their place at the time of the bombing (Table 1).
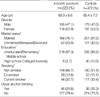
No significant differences in average age, gender ratio, and alcohol consumption frequency occurred between the survivors and controls. However, marital status (p<0.05), education (p<0.01), and smoking status (p<0.01) differed significantly between the two groups. More of the survivors were married and less well educated than the controls, but there were fewer current smokers among the survivors.
The univariate analysis revealed significantly lower fasting glucose and creatinine levels in the survivors. Conversely, diastolic blood pressure (DBP), serum AST, ALT, and BUN were higher in the survivors (Table 3).
Except for DM+IGT, A-bomb survivors had a higher prevalence of non-cancer diseases than controls. The calculation of crude PRs revealed that A-bomb survivors had a significantly higher prevalence of hypertension (PR, 1.16; 95% CI, 1.00-1.35) and chronic liver disease (2.20; 1.59-3.06) than controls. After adjusting for covariates, A-bomb survivors had a significantly higher prevalence of hypertension (1.24; 1.06-1.44), chronic liver disease (2.07; 1.51-2.84), and hypercholesterolemia (1.79; 1.11-2.90) than controls (Table 4).
DISCUSSION
U.S.A. and Japanese scientists have consecutively developed dosimetry systems, i.e., T65D (Tentative 1965 Radiation Dose Estimates for Atomic Bomb Survivors), DS86 (Dosimetry System 1986), and DS02 (Dosimetry System 2002), to determine the radiation doses of Japanese A-bomb survivors(12). In Japan, information regarding individual A-bomb exposure histories, such as each survivor's location and detailed shielding situation at the time of the bombing, was obtained through interviews conducted during the late 1950s and early 1960s. Based on these data and dosimetry systems derived from theories of modern nuclear physics, individual radiation dose estimates are presently available for 92% of the approximately 100,000 Japanese A-bomb survivor cohort
and about 80% of those who were exposed within 2 km of the hypocenters (13). On the contrary, a scientific and systematic survey of A-bomb exposure histories of Korean survivors has never been conducted in Korea. The majority of survivors were exposed to the A-bomb during childhood or adolescence, and 59 yr had passed before we conducted this study. Thus, survivors had difficulty in accurately recalling their location and situation at the time of the bombing despite our efforts to stimulate their memory, which inevitably led the exposure assessment of this study to contrast A-bomb survivors with non-exposed controls.
The clinical indicators of non-cancer diseases evaluated in this study were well standardized and easily measured at a majority of the hospitals and clinics in Korea. Thus, discrepancy between examiners and examining methods of the clinical indicators of the survivors and controls did not violate the comparability of the two groups.
In the analysis of data from cross-sectional studies, two ratio measures of effect have been used: the prevalence odds ratio (POR) and the prevalence ratio (PR). Although there is no dispute that the PR and POR will be similar for a rare disease, they may produce a discrepancy for a common disease. When analyzing common diseases, the POR generally produces higher estimates with wider confidence intervals than the PR (14). Therefore, we calculated the PRs of non-cancer diseases in this study.
Shimizu et al. reported that mortality from hypertensive heart disease among Japanese A-bomb survivors increased with the radiation dose (15), and Sasaki et al. reported that atomic bomb exposure was related to elevated blood pressure (16). Akahoshi et al. reported that the atomic-bomb radiation dose was positively related to fatty liver identified by abdominal ultrasonography, low HDL-cholesterol, and hypertriglyceridemia and that these relationships were independent of age, sex, BMI, smoking, and drinking habits (17). In the Japanese A-bomb survivor cohort, the mean growth curve of serum cholesterol levels from 1958 to 1986 for irradiated individuals was significantly higher than that for non-irradiated controls, in both men and women (18). In addition, an excess risk of non-cancer diseases after exposure to radiation has also been reported. Patients who received radiotherapy for Hodgkin's disease (19) or breast cancer (20) have shown an increased risk of mortality from cardiovascular disease. The analysis of Russian workers involved in the clean-up following the Chernobyl accident provides some indication of the increase in the incidence of, but not mortality from, non-cancer diseases (21). In this study, atomic bomb exposure had a positive association with prevalence of hypertension, chronic liver disease, and hypercholesterolemia. These results concur with previous findings of non-cancer diseases in those exposed to radiation. Target organ damage and the induction of atherogenesis or inflammatory markers, such as C-reactive protein, interleukin-6, and other markers, have been hypothesized as mechanisms of non-cancer diseases by radiation exposure (22-24). However, the possible biological mechanisms that cause excess risk of non-cancer diseases are still unclear.
We found no significant association between atomic bomb exposure and impaired glucose metabolism (DM+IGT). Nor has any correlation been reported between the prevalence of DM and the radiation dose at Hiroshima and Nagasaki (25,26). However, in a study using unpublished data, Wong et al. reported that the prevalence of DM, diagnosed on the basis of medical history and measurements of blood glucose and glycosylated hemoglobin (hemoglobin A1c), was significantly higher among Hiroshima females under the age of 20 yr who were exposed to high doses of radiation (18). Thus, further studies are needed to confirm the association between radiation and glucose metabolism.
The Korean survivors were less educated than the controls (Table 2). A low level of education is generally related to low socioeconomic status (SES), and low SES is related to poor health. Both atomic bomb exposure and low SES may have contributed to the health status of the survivors. Most of the survivors were exposed to the atomic bomb during childhood, which means that their parents were also exposed. The poor health of both the survivors and their parents caused by atomic bomb exposure may have contributed to their lack of education. We believe that the low level of education of the survivors is inseparable from atomic bomb exposure.
Our study was limited to the survivors in residence at Hapcheon. Although this was not a random sample of Korean survivors, it is unlikely that residing at Hapcheon caused an unusual selection of survivors with non-cancer diseases and distorted the relationship between A-bomb exposure and prevalence of non-cancer diseases. Further study evaluating the health of all Korean survivors needs to be conducted. We did not evaluate the nutritional status of the survivors. The clinical indicators evaluated in this study are related to nutrition, but further nutritional evaluations are needed. As this study was cross-sectional, future trends in the health of the survivors cannot be predicted without longitudinal follow-ups. Finally, this study did not investigate malignancy in the survivors, and further study of this is also needed.
This study suggests that A-bomb exposure is associated with a higher prevalence of non-cancer diseases in Korean survivors. Although many years have passed since the detonation of the atomic bombs, health concerns related to atomic bomb exposure are still being raised (27-29). Additional studies investigating the health of Korean A-bomb survivors are needed.



 XML Download
XML Download