

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prostate cancer is the sixth most common malignancy in Korean men. It accounts for approximately 3% of all newly diagnosed cases of cancer patients among men. The incidence of prostate cancer has significantly increased during the past decade (1).
Men who are newly diagnosed with prostate cancer receive various treatment modalities based on the stage of disease. Since prostate cancer is characterized by slowly growing tumors, and is usually diagnosed in elderly males, individual health-related quality of life (HRQOL) is an increasingly important consideration with respect to treatment (2).
Cella and colleagues (3) developed the Functional Assessment of Cancer Therapy-General (FACT-G). It has a well-established validity and reliability (3-6), and has been widely used to measure the HRQOL in cancer patients. However, since the FACT-G has included comprehensive and general HRQOL items, disease-specific subscales of the FACT have been introduced. Subsequently, the development and validation of a prostate cancer subscale have been described (7, 8). Thus, the Functional Assessment of Cancer Therapy-Prostate (FACT-P) consists of FACT-G and a prostate cancer subscale.
The Korean FACT-G had been previously translated (access http://www.facit.org for details) and validated (6, 9, 10). However, the prostate cancer subscale had not been translated into Korean. Therefore, we present the results of a study that was performed to translate and validate the Korean FACT-P questionnaire.
MATERIALS AND METHODS
Development of the Korean FACT-P
The Korean version of the FACT-P was developed from the English FACT-P, which was provided by the Center on Outcomes, Research and Education (CORE), at Evanston Northwestern Healthcare (Evanston, IL, U.S.A.). The initial procedure was a double back-translation of the prostate cancer subscale, according to a previously described method (11), which was performed in the following sequence. Step 1: forward translations by two native Korean translators. Step 2: reconciliation of the forward translations by another native Korean translator, who was not involved in step 1. Step 3: back-translation of the reconciled version by a native English speaker, who was also fluent in Korean. Step 4: independent reviews by 3 bilingual experts, which included two experts with knowledge of medical concepts and one language coordinator, who completed the most suitable translation for each item from the forward or reconciled forms and/or provided alternative translations if necessary. Step 5: finalization by the Functional Assessment of Chronic Illness Therapy (FACIT) translations project team. Step 6: formatting and proofreading of the new translation for pilot testing on native Koreans who were prostate cancer patients.
The revised Korean version was tested on 15 Korean prostate cancer patients at the Samsung Medical Center, in Seoul. The purpose of this pre-test was to determine whether any items were difficult to understand or culturally irrelevant. All comments made by the patients regarding comprehension of each item were recorded. There was no item to which they felt uneasy responding. The final Korean FACT-P (Version 4) was then completed, following statistical confirmation by the FACIT translations project team.
Testing of reliability and validity
A total of 70 consecutive prostate cancer patients, who underwent curative or palliative treatment, were identified as the cohort of a validation test in an outpatient setting. In addition, an equal number of age-matched controls were selected to compare with the results of the FACT-P in the cancer patients. The data from the controls were obtained when they visited either the Center for Health Promotion or the outpatient center of the Department of Urology at Samsung Medical Center. The exclusion criteria for the controls were: a previous, or current, history of another malignancy; age less than 50 yr old; serum level of prostate-specific antigen (PSA) ≥2.5 ng/mL; and/or a chronic debilitating disease. Our institutional research ethics board approved the study protocol. All the subjects provided their fully informed consents.
To estimate test-retest reliability, the Korean FACT-P questionnaire was administered twice to each cancer patient after an interval of one week. After each patient submitted the first questionnaire in an outpatient center, a second questionnaire was submitted by mail.
Statistical analyses
The statistical analyses for the reliability and validity of the FACT-P were performed using SPSS for Windows (Version 10.0; SPSS, Chicago, IL, U.S.A.). The internal consistency of each subscale was estimated by using Cronbach's alpha coefficient. The test-retest reliability was estimated by calculating intraclass correlation coefficients of the subscales between the initial and subsequent measured questionnaires.
Construct validity was estimated from the inter-subscale correlation by using Spearman's correlation. The differences between the FACT-P scores of the cancer patients and the controls were calculated by Student t-test and Wilcoxon ranksum test.
RESULTS
A descriptive analysis of the baseline characteristics of the cancer patients is demonstrated in Table 1. The median time following a diagnosis of cancer was 23 months (range, 2-115 months). More than 98% of the patients had a favorable performance status rating in our study.
The age distribution between the cancer patients and the controls was similar, with an average age of 66.1 and 64.5 yr old, respectively (p=0.160). The mean PSA value in the controls was 1.2±0.5 ng/mL. The controls completed the questionnaires either in the Center for Health Promotion (23 men, 33%) or the outpatient center of the Department of Urology (47 men, 67%).
The mean scores of the FACT-P subscale, along with Cronbach's alpha coefficients, are presented in Table 2. In addition, the English FACT-P scores are detailed. Cronbach's alpha coefficients for the individual subscales were 0.7 or greater, except for emotional well-being. Internal consistency of the FACT-G and FACT-P totals was both high. Cronbach's alpha coefficient for the FACT-G, was 0.86, and for the FACT-P, was 0.88.
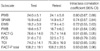
Table 3 demonstrates that test-retest reliability was high for physical well-being, functional well-being, FACT-G, prostate cancer subscale, trial outcome index, and the FACT-P total (intraclass correlation coefficients were greater than 0.80). Moderately high correlations were observed for emotional well-being and social/family well-being (with coefficients of 0.72 and 0.74).
Table 4 demonstrates the inter-subscale correlations. It has been hypothesized that a correlation coefficient greater than 0.40 between subscales, indicated that the two were conceptually related (12). In the FACT-G subscales, the highest correlation was observed between social/family well-being and functional well-being subscales, but the correlation was modest (r=0.56). The other correlations were less than 0.4, inferring that each subscale of the FACT-G was unrelated. However, other high correlations were observed not only between the prostate cancer subscale and physical well-being (r=0.64), but also between the prostate cancer subscale and functional well-being (r=0.45). The reason was that the prostate cancer subscale had some degree of overlapping items compared with the other subscales, especially in the case of physical well-being.
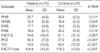
The ability of the FACT-P scale to discriminate reliably between the cancer patients and the age-matched controls was assessed by comparing the responses from the two groups. Table 5 demonstrates that highly significant differences were observed between the cancer patients and the controls for most subscales. The least degree of difference between the cancer patients and the controls was observed with emotional well-being, where the results failed to reach statistical significance. There were significant differences between the cancer patients and the controls in half (20 items) of the total 39 items. The cancer patients usually suffered from pain, erectile dysfunction, distress, and dissatisfaction.
DISCUSSION
Men, with either localized or advanced prostate cancer, face a range of treatment options associated with disturbing side effects and functional impairments (13). Although the primary endpoint of treatment for prostate cancer remains to eliminate disease progression and maximize survival, HRQOL is recognized increasingly as an important outcome of any treatment modality (2, 13, 14). In fact, the incidence of prostate cancer has dramatically increased during the past decade in Korea. However, no prostate cancer-specific HRQOL measurement had previously been developed and validated in a clinical setting.
There are many questionnaires available to measure the HRQOL of patients with prostate cancer (2). The FACIT questionnaires are among those more commonly used for various cancers and chronic illnesses in research settings. The FACIT are an expansion of the familiar FACT questionnaires into other chronic illnesses and conditions.
The FACT-G (Version 4) contains a 27-item questionnaire and is composed of four subscales of HRQOL: physical well-being (PWB), social/family well-being (SFWB), emotional well-being (EWB), and functional well-being (FWB) (6, 15). The prostate cancer subscale (PCS) is composed of a 12-item issue, related to prostate-specific questions, which include sexuality, bowel/bladder function, and pain. Equivalent versions of the FACT-P questionnaires are available in 20 different languages, which permit cross-cultural comparisons of people from diverse backgrounds (6). Therefore, the FACT-P questionnaire is considered to be a relevant measurement for assessing the health-related quality of life in men with prostate cancer.
This study described the method used to translate and validate the FACT-P from its original English language into Korean.
Generally, the customary ranges of Cronbach's alpha coefficient are identified as acceptable (0.60 to 0.69), good (0.70 to 0.79), and high (0.80 to 1.0) levels. The translated Korean-language version appeared to perform at least as well as the original English form, with comparable reliability coefficients (7). With the exception of the emotional well-being subscale (Cronbach's alpha coefficient=0.61), internal consistency coefficients were all greater than 0.70. The item GE2, I am satisfied with how I am coping with my illness, showed significantly low inter-item correlation in the emotional well-being subscale. The translated term for 'coping' is not commonly used in community basis. About 34% of patients are more than 70 yr old and 14% were not graduated from middle school in this study. Therefore, they might have a problem for understanding the meaning of coping. Test-retest repeatability correlation coefficients ranged from 0.72 to 0.93, and were all highly significant. Overall, the FACT-P demonstrated a strong internal consistency, measured in terms of both the total scale and individual domain scores, and adequate test-retest reliability.
The inter-subscale correlations demonstrated that there was a modest relationship between social/family well-being and functional well-being subscales in this study. This result may be due to a unique characteristic of the enrolled patients. That is, since almost of the cancer patients in this study had a favorable performance status, they were not likely to have been disturbed by the disease itself. Therefore, the functional status of these patients was good, and they were able to perform their social roles in their relationships with friends and families.
For the discriminant validity test, analyses were performed in each of these areas in two separate samples of the cancer patients and the age-matched controls. The differences between the two groups were significant for all subscales, with the exception of emotional well-being. Therefore, the FACT-P questionnaire can reliably differentiate between the cancer patients and the controls in the clinical practice.
The relatively small sample sizes and selection of cancer patients are recognized limitations of this study. Our cancer cohort is exclusively interviewed in outpatient setting, and thus patients with good performance status were participated in this study. Therefore, our results may not represent the characteristics of whole prostate cancer patients in Korea. Thus, further studies are needed with large sampled populations and various performance statuses.
In conclusion, the Korean translation of the FACT-P questionnaire was developed and verified in its reliability and validity. This instrument can be used as a reliable self-administrated scale for assessing HRQOL in patients with prostate cancer in both the clinical and research fields.



 XML Download
XML Download