

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Among the general population, it has been assumed that an average of 150 to 250 µg of lead is ingested through food each day, five to ten percent of which is absorbed (1, 2). The other sources for lead poisoning may be lead-soldered kettles, cans, and lead-glazed pottery, which release lead when acidic fluids are stored or cooked in them (2).
The lead in blood is equilibrated with that of lead in tissues, including many potential target organs such as the brain and kidney. The kinetic model of lead in the body is not defined well, but usually it consists of two pools: in the blood and in the skeleton, which may be divided further into labile and deep pools (3). The kidney is the main organ excreting lead from pool. Thus, lead burdens have a tendency to be accumulated in the patients with renal failure (4).
The skeleton acts as a reservoir of lead, and it may be mobilized by physiological and pathological states including pregnancy, lactation, and osteoporosis (5, 6). In patients with end-stage renal disease (ESRD), hyperparathyroidism, abnormal vitamin D metabolism, and consequent osteoporosis have frequently been observed (7). Taken together with the lack of renal excretion and stimulated bone resorption, the blood level of lead seems to increase in ESRD and may aggravate uremic symptoms such as peripheral neuropathy and anemia.
The classic clinical manifestations of industrial lead poisoning include colic, anemia, peripheral neuropathy, encephalopathy, renal impairment, hypertension, and reproductive disability (8). More recently, recognition has become widespread that, in addition to its clinically evident toxicity, lead also causes a spectrum of adverse effects at levels of exposure insufficient to produce obvious signs and symptoms. The premise underlying this recognition is that there exist asymptotic, subclinical counterparts. Thus, clinically obvious manifestations of lead poisoning such as anemia, peripheral neuropathy, and renal failure lie at the upper end of the range of toxicity, while such covert effects as impaired synthesis of heme, altered excretion of uric acid, and slowed nerve conduction are their subclinical correlate (9).
Diseases of the peripheral nervous system are among the most prevalent neurologic conditions in ESRD (10). Nonetheless, differential diagnosis of peripheral nerve disease is challenging because the catalogue of disorders that can produce neuropathies is extensive in ESRD. First of all, many patients with renal failure develop electrophysiologic evidence of peripheral neuropathy (11). The primary pathophysiology of uremic neuropathy remains unknown. According to one theory (12), some slowly dializable substances of intermediate molecular weight alter the peripheral nerve in some manner, resulting in axonal dysfunction and eventually degeneration. The other causes of the peripheral neuropathy in ESRD are diabetes mellitus, pharmaceutic neurotoxins, alcohol-nutritional neuropathy, and industrial and environmental neurotoxins such as lead, mercury, arsenic, and thallium.
Although many investigators have described increased blood levels of lead in renal failure patients (13-16), the role of lead on the clinical characteristics remains to be elucidated. The purpose of this study is to determine the blood concentration of lead in patients with end-stage renal disease and to validate the relation with peripheral motor and sensory nerve conduction velocity as clinical correlates.
MATERIALS AND METHODS
Subjects
One hundred ninety-eight healthy subjects (control group, 147 men, 51 women; mean age, 43.2±11.5 yr) and 68 patients with ESRD undergoing hemodialysis (ESRD group, 31 men, 37 women; mean age, 50.1±12.3 yr) were enrolled for the blood lead measurement. The control group comprised healthy volunteers recruited during a regular physical examination at Soonchunhyang University Health Promotion Center (Cheonan, Korea). Blood samples for lead concentration were drawn from the antecubital vein in the morning after overnight fasting.
The ESRD patients were undergoing regular hemodialysis eight to twelve hours weekly using a cellulose acetate hollow-fiber dialyser (surface area 1.2 m2; Gambro, Sweden, or Baxter, U.S.A.) at a hemodialysis unit of the Soonchunhyang Cheonan Hospital. In order to avoid any influence of carpal tunnel syndrome and/or ischemic neuropathy on the result of peripheral nerve conduction study, any patients who had vascular access on the right arm and had past histories of cerebrovascular disease, with or without hemiparesis, were excluded from this study. Among 124 ESRD patients on hemodialysis, 68 cases were consistent with these terms.
This study was approved by the Institutional Review Board of Soonchunhyang Cheonan Hospital (Cheonan, Korea), and all human subjects provided written informed consent
Measurement of nerve conduction velocity
Nerve conduction was measured within two hours after hemodialysis. The upper limb temperatures were maintained above 34℃ and lower limb temperatures above 32℃, using hot packs when necessary. Orthodromic sensory nerve action potentials and compound muscle action potentials were recorded in response to supramaximal constant-voltage stimulation (duration=0.1 msec; sensory=20 mA, motor=25-35 mA). Stimuli were delivered from a bipolar stimulator; stimulating electrodes were 0.8 cm in diameter, and their centers separated by 1.8 cm. Motor and sensory responses were recorded with 0.8 cm disk electrodes. The amplifier band pass was 2-10.000 Hz for all nerve conduction study. A Dantec Keypoint version 2.0 electrodiagnostic system (Dantec Com, Skovlunde, Denmark) was employed. Studies were performed by two physicians among the authors and were assisted by a technologist.
For excluding idiopathic carpal tunnel syndrome, which could also be caused by diabetes and uremia, we included both the motor conduction study in the wrist-elbow segment of the median and ulnar nerves and the motor and sensory conduction studies in the radial nerve. Results were compared with age-specific normative data obtained in the same laboratory.
Measurement of blood lead concentration
Blood samples for lead level, CBC, and general chemistry were drawn from a venous line at the beginning of hemodialysis. Blood lead level was analyzed in duplicate with a Zeeman background-corrected atomic absorption spectrophotometer (Hitachi Z-8100, Japan) with NIOSH's standard addition method (17) at Soonchunhyang University Institute of Industrial Medicine, a certified reference laboratory for lead in Korea.
Statistical analysis
Data were presented as a mean (SD) for continuous variables and frequency (%) for categorical variables. Pearson's correlation was applied between outcomes and covariates. Multiple linear regression was used to determine associations between blood lead and nerve conduction tests, adjusting for potential confounders. For easy presentation of results, the final regression models were selected with the same set of confounding variables (i.e., age, sex, duration of hemodialysis, Kt/V, and protein catabolic rate). All models were evaluated for violation of the assumptions of linear regression. A value of p<0.05 was considered statistically significant, and all statistical analysis was performed using a Stata program (Stata Release 5, College Station, Texas, U.S.A.).
RESULTS
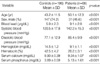
In the control group, mean systolic and diastolic blood pressure were 120.5±17.8 mmHg and 77.1±12.9 mmHg, respectively. Hemoglobin and hematocrit were 14.5±2.2 mg/dL and 42.5±4.2%. Serum calcium and phosphorus were 9.9±0.39 mg/dL and 3.89±0.59 mg/dL (Table 1).
In ESRD group, the median duration of hemodialysis was 42.5 months (range; 1 to 210 months). The causes of renal disease were diabetes mellitus (n=22), hypertension (n=20), polycystic kidney disease (n=1), glomerulonephritis (n=20), and unknown factors (n=7). Kt/V was 1.30±0.27. Normalized protein catabolic rate (nPCR) was 1.2±0.2. Mean systolic blood pressure was 142.2±15.5 mmHg, and mean diastolic blood pressure was 85.4±9.9 mmHg. Sixty two of 68 patients have had anti-hypertensive medications. Seventeen cases (25%) were current smokers and 8 patients (11.8%) were regular drinkers (Table 2). The mean serum albumin level was 3.7±0.4 g/dL. Hemoglobin was 9.1±1.1 mg/dL and hematocrit was 26.2±3.1%. Serum calcium and phosphorus were 9.34±1.07 mg/dL and 5.13±1.61 mg/dL, respectively.
Blood lead levels were corrected by hemoglobin (15 mg/dL) in both groups, and compared. After the correction, blood lead levels were significantly higher in the ESRD group than in control group (p<0.001). All other study variables were significantly different between the groups (p<0.001) (Table 1). Summary of nerve conduction tests is displayed in Fig. 1. Blood lead was significantly correlated with duration of hemodialysis (p<0.05) (Table 3). However, other study variables were not related to blood lead. Also, motor or sensory nerve conduction velocity did not show significant correlation with blood lead in ESRD patients (Table 4). The positive correlation was observed between nutritional marker, nPCR, and ulnar motor nerve conduction velocity. Also, the positive correlation was observed between duration and radial sensory nerve conduction velocity.
In the final models, blood lead was not a significant predictor of poor nerve conduction velocity. Patients with diabetes mellitus showed significantly worse motor and sensory function in all three nerves than those without diabetes mellitus (p<0.01) (Table 5).
DISCUSSION
Lead poisoning may remain asymptomatic for many years. Major forms of lead poisoning are lead colic, hypertension, and neuropathy. On the other hand, minor symptoms are common and variable: cramps, paresthesia, intermittent pain in the limbs, chronic abdominal pain, and functional digestive disturbances. It is not easy to define these symptoms in patients with ESRD because uremia itself may cause of and/or aggravate these symptoms. Furthermore, chronic lead poisoning may be a cause ESRD (18-21). The design of our study does not enable us to discuss the role of lead overload in the onset of ESRD. Determination of such a relationship would require epidemiological studies conducted according to rigorous methodology.
In our results, the blood lead levels were significantly higher, almost twice that of the control group (9.1±2.8 µg/dL vs. 5.9±2.3 µg/dL) in ESRD patients. However, contrary to our expectation, there was no correlation between the blood lead levels and peripheral nerve conduction. Of course, there are many factors influencing the peripheral nerve conduction in ESRD. Approximately 60% of patients with renal failure develop electrophysiologic evidence of peripheral neuropathy (22). The pathophysiology of uremic neuropathy remains unknown. Some slowly dializable substances of intermediate molecular weight have been proposed as pathogens, resulting in axonal dysfunction and eventually degeneration (12). With this point of view, heterogeneity of adequacy in hemodialysis may influence the nerve conduction. But in our study, the Kt/V was 1.30±0.27, and there was no correlation between Kt/V and peripheral nerve conduction.
Another problem during the evaluation of peripheral nerve conduction is the possibility of carpal tunnel syndrome in patients with ESRD. It is well known that patients with ESRD are apt to suffer from carpal tunnel syndrome (23-25), which may mask the results of peripheral nerve conduction study. The carpal tunnel syndrome is related to a small β2 microglobulin that normally is catabolized by the healthy kidney (26, 27). This substance forms a type of amyloid deposit throughout the body, with particularly adverse consequences when it is deposited in the carpal tunnel about the transverse carpal ligament. On the other hand, a profound combined ischemic neuropathy, referred to as an ischemic monomelic neuropathy, may result in patients with limb ischemia secondary to shunt (22, 28). A significant combined neuropathy may be associated with loss of sensation and muscle weakness in the distal arm supplied by the shunted vessels. In order to avoid any influence of carpal tunnel syndrome and/or ischemic neuropathy on the result of our peripheral nerve conduction study, we performed the motor conduction study on the wrist-elbow segment of the median and ulnar nerves, and the motor and sensory conduction studies on the radial nerve in the right arm. Any patients who have vascular access in the right arm were excluded from this study.
Alcohol and nutrition are also important factors in peripheral neuropathy in ESRD (22). In our results, both sensory nerve action potentials and compound muscle action potentials were significantly more suppressed in patients with diabetes mellitus than in the non-diabetes mellitus group. The nutritional markers of nPCR (1.03±0.38) and serum albumin level (3.7±0.4 g/dL) were relatively homogenous among the patients with hemodialysis. In our result, positive correlation was observed between nPCR and ulnar motor nerve conduction. But the other nerve was not correlated. We guess that malnutrition is important factor about nerve conduction in ESRD patient, but only decreased nPCR may be no prognostic marker about nerve conduction.
The other causes of peripheral neuropathy in ESRD are pharmaceutic neurotoxins and industrial and environmental neurotoxins such as mercury, arsenic, and thallium (22). We did not measure such metals. Further studies are needed for evaluation of peripheral neuropathy in ESRD.
Of course, there is a possibility that the blood lead levels are not high enough to produce the neuropathy in ESRD patients. In the peripheral nervous system, the motor axons are the principal target of lead. Lead-induced pathologic changes in these fibers include segmental demyelination and axonal degeneration (29). Recent studies of the peripheral nerves in persons exposed to lead have used electrophysiologic probes to determine whether lead causes covert abnormalities in function. They found slowed conduction in the small motor fibers of the ulnar nerve to be the most sensitive peripheral index of the neurotoxicity of lead and the ulnar nerve conduction velocity was depressed at blood levels below 50 µg/dL. In conjunction with this report, our result reveals that, even though the blood lead levels were high in ESRD, they were still below the level of inducing peripheral neuropathy.





 XML Download
XML Download