

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Arteriosclerotic change of radial artery in hemodialysis (HD) patients is known as an important risk factor of vascular access failure (1, 2). We have reported that intimal hyperplasia (IH), which is the main pathologic change of radial artery, is associated with early failure of radiocephalic arteriovenous fistula (AVF) in HD patients (3). But, there is no noninvasive method to predict IH of radial artery before the vascular access operation.
Ultrasonography is considered as a fundamental technique to investigate the vascular system, especially carotid artery (4-6). The intima-media thickness (IMT), which represents whole thickness of arterial wall, can be measured by ultrasonography. However, the intima thickness is exceptional. We have reported that radial arterial IMT measured by ultrasonographic examination was correlated well by histological examination (7). This study was performed to evaluate the impact of IMT on the early failure of AVF in HD patients by histologic examination.
MATERIALS AND METHODS
Patient population
One hundred twenty-six uremic patients underwent radiocephalic AVF operation for the first time at our hospital between January 2000 and December 2003. We selected radiocephalic AVF as the first choice of vascular access type. However, when the cephalic vein was too small to create a radiocephalic AVF or collapsed because of recent multiple punctures, we placed other vascular accesses (upper arm AVF, AV graft, central catheter). Of these patients having radiocephalic AVF, this study included the patients who underwent radial artery biopsy during the surgery. To avoid vessel injury before the operation as a cause of early AVF failure, we excluded patients who had a history of central venous cannulation or arterial puncture ipsilateral to the AVF surgical site. As a result, total 90 patients who were fit with these criteria and included in this study. This study was approved by the Institutional Review Board of Uijongbu St. Mary's Hospital.
Measurement of wall thickness of radial artery
A radiocephalic AVF was constructed in an end vein-to-side artery fashion at the wrist by a single vascular surgeon. During the operation, 10-mm long partial arterial walls were removed from the incision sites of the radial arteries with elliptical form for microscopic analysis. Specimens were cut into 5-µm sections and stained with hematoxylin and eosin and trichrome. Slides were examined by a pathologist blinded to the clinical data. The each wall thickness of radial artery (intima, media, and intima-media thickness) was measured using light microscopy respectively and atherosclerotic lesion was investigated. An atherosclerotic lesion was defined as the presence of cholesterol clefts or aggregation of foamy macrophages. The IMT was defined as sum of intima thickness and media thickness and IH was defined as the presence of cells and fibrous tissues between the endothelium and internal elastic lamina as our previous study (3).
Follow-up of AVF patency
Before the operation, we investigated hypertension, smoking history, hemoglobin, hematocrit, serum cholesterol, total protein, and albumin level. AVF patency was prospectively followed up for 1 yr after the operation. First cannulation through the AVF for hemodialysis was individualized according to the state of venous maturation at least 4 weeks after the operation. If hemodiaysis treatment had been needed before venous maturation, the catheter for hemodialysis was inserted at the central vein contralateral to the AVF site and hemodialysis was performed. We investigated early AVF failure within 1 yr after the operation. Early AVF failure was defined as complete obstruction or low blood flow insufficient to support a dialysis flow rate of at least 200 mL/min and require radiologic intervention or surgical correction within 1 yr after the operation as our previous study (8). Of the AVF failures that occurred in this study, nonthrombotic events such as those caused by infection or external compression were excluded. AVF failure caused by external compression was defined as cessation of blood flow just after prolonged compression of the needling sites of AVF. We compared clinical factors and each wall thickness of radial artery between failed and patent group. And we also evaluated relationship between the AVF failure and radial artery IMT or IH.
Statistical analyses
A comparison of mean value of the clinical factors and each wall thickness according to the radial artery IMT values or AVF patency was made by using unpaired Student t test. For comparison of AVF patency between patients with IMT <500 µm and ≥500 µm and between patients with and without IH according to the time course survival analysis using Kaplan-Meier method with log rank test was performed. To decide independent risk factors of IMT and early AVF failure out of the clinical factors, multiple regression analysis and Cox regression analysis were used, respectively. When comprising groups, p less than 0.05 is considered to be significant.
RESULTS
Clinical characteristics
Mean age of the patients was 56±13 yr and the number of female was 44 (48.9%). Primary renal diseases consisted of diabetic nephropathy (52 cases), chronic glomerulonephritis (19 cases), hypertensive nephropathy (11 cases), polycystic kidney disease (3 case), Goodpasture's disease (1 case), and unknown (4 cases). The percentage of hypertension and smoking history was 75% (n=68), 40% (n=36), respectively. Mean hemoglobin level and hematocrit were 8.8±1.2 g/dL, 26.0±3.9%, respectively. Serum albumin and total cholesterol levels were 3.1±0.5 g/dL, 178±52 mg/dL, respectively.
Each wall thickness of radial artery and incidence of IH and atherosclerotic lesion
Mean intima thickness was 57±42 µm (13-225 µm) and mean media thickness was 376±120 µm (120-700 µm). Mean IMT, which is sum of intima thickness and media thickness, was 430±132 µm (133-760 µm). Of the total 90 patients, 8 patients had normal range of IMT (less than 250 µm) and 82 patients had increased IMT (more than 250 µm). Of the 82 patients with increased IMT, 56 patients had IMT more than 250 µm and less than 500 µm and 26 patients had IMT more than 500 µm. IH was observed in 67 of the total 90 patients (74%) and atherosclerotic lesion was found in only two patients.
Comparison of each wall thickness of radial artery between patent and failed groups
During follow up for 1 yr after the operation, there was no any follow-up loss. Four patients died with AVF failure and 5 patients died with patent AVF before the end point of this study. In comparison of each wall thickness of radial artery, we excluded 5 patients who died with patent AVF before the end point of this study. Of the total 90 patients, 31 patients (34%) had AVF failure within 1 yr after the operation. Eighteen of the 31 AVF failures occurred within 4 months after the operation. Except 5 patients who died with patent AVF, we compared each wall thickness of radial artery between patent group (n=54) and failed group (n=31). Mean intima thickness, media thickness, and IMT were thicker in failed group than in patents group, respectively (intima thickness; 75±34 µm vs. 45±38 µm, p=0.001, media thickness; 413±126 µm vs. 355±116 µm, p=0.042, IMT; 486±130 µm vs. 398±130 µm, p=0.004) (Fig. 1).
Comparison of age, and incidence of diabetes mellitus and hypertension between patent and failed groups
We compared age, incidences of diabetes mellitus and hypertension between patent and failed groups. Of the total patients, we also excluded 5 patients who died with patent AVF before the end point of this study. Mean age in the failed group was older than that in the patent group (61±10 yr vs. 53±15 yr, p=0.011). The incidence of diabetes mellitus in the failed group tended to be higher than that in the patent group but the difference was not significant (43% vs. 27%, p=0.154). There was no difference in the incidence of hypertension between the 2 groups (35% vs. 37%, p=0.876).
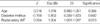
Cox regression analysis for the independent clinical factors affecting early AVF failure
To evaluate the independent risk factors of early AVF failure, we analyzed age, diabetes mellitus, and IMT value using Cox regression analysis. Expired cases were dealt with censored data. Of these clinical factors, only IMT was independent risk factor of early AVF (Table 1).
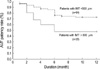
Comparison of AVF patency according to radial artery IMT and IH
Using a threshold of 500 µm of IMT, AVF patency rate was compared between these two groups using Kaplan-Meier method with log rank test. Expired cases were dealt with censored data. The AVF patency rate within 1 yr after the operation was lower in patients with IMT ≥500 µm (n=26) than in patients with IMT <500 µm (n=64) (p=0.017, Fig. 2). The AVF patency rate in patients with IH (n=67) was also lower than in patients without IH (n=23) (p=0.041).
Comparison of clinical factors between the patients with IMT ≥500 µm and <500 µm
The patients with IMT ≥500 µm was older and had higher incidence of diabetes mellitus, compared to the patients with IMT <500 µm (Age; 62±9 vs. 54±14 yr, p=0.006, incidence of diabetes mellitus; 77% vs. 50%, p=0.019). But there was no difference in sex, smoking, hypertension, hemoglobin, hematocrit, serum total cholesterol and total protein, and albumin levels between the two groups (Table 2).
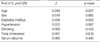
Multiple regression analysis for the independent clinical factors affecting IMT
To evaluate the independent risk factor of IMT, we analyzed the clinical factors, age, sex, diabletes mellitus, hypertension, smoking history, serum cholesterol, and albumin level, using multiple regression analysis. Of these clinical factors, only age was independent risk factor of IMT. Diabetes mellitus tended to be independent risk factor but not statistically significant (Table 3).
DISCUSSION
This study first demonstrated the association between the radial artery IMT measured by histologic examination and early failure of radiocephalic AVF in HD patients. The causes of early failure of radiocephalic AVF are often unknown although the quality of the radial artery is thought to play an important role. The IMT represents whole thickness of arterial wall, which can be measured by high-resolution ultrasonography (4-6). We previously reported that ultrasonography is accurate in measuring radial artery IMT, compared to histologic examination (7). Although radial artery IMT, which represents actual wall of the radial artery, is considered to play an important role of early failure of radiocephalic AVF, the impact of the radial artery IMT on the early failure of radiocephalic AVF is not reported yet.
We previously reported that preexisting IH of the radial artery is associated with early failure of radiocephalic AVF in hemodialysis patients (3). However, IH can be detected only by histologic examination during the operation and there was no available noninvasive method to measure it directly. It cannot be helpful for the surgeon to decide which the radial artery is an adequate for the radiocephalic AVF or not. Carotid artery IMT can be easily measured by high-resolution ultrasonography and increased carotid artery IMT is known to be an independent risk factor of cardiovascular morbidity and mortality (4-6). Mackay et al. (9) reported that radial artery IMT in patients with severe coronary artery atherosclerosis awaiting coronary artery bypass grafting was thicker than that in healthy persons. We also reported that radial artery IMT in uremic patients was thicker than that in both uncomplicated hypertensive patients and healthy persons (7). Based on these findings, we hypothesized that radial artery IMT would be associated with early failure of the radiocephalic AVF and retrospectively evaluated radial artery IMT by using histologic examination in uremic patients who received radiocephalic AVF operation and investigated early failure of the radiocephalic AVF within 1 yr after the operation. Patients with IMT ≥500 µm had lower patency rate within 1 yr after the operation than patients with IMT <500 µm (p<0.001). Our findings suggest that increased radial artery IMT may be one of the factors of early failure of radiocephalic AVF in HD patients. Therefore, we recommend that ultrsonography should be performed in pre-dialysis uremic patients having poor vascularity prior to the radiocephalic AVF creation. In patients with radial artery IMT ≥500 µm, the radiocephalic AVF operation should be avoided and other types of vascular access such as brachiocephalic AVF or graft should be considered.
Because it is clinically difficult to obtain the radial artery specimens, there are few data about histologic study of the radial artery. The main pathologic derangement of the radial artery is IH and role of atherosclerosis is strictly restricted, in contrast to carotid and coronary arteries in which atherosclerosis commonly occur (3, 10-12). Ejerblad et al. (10) found that IH in the radial artery was observed in all uremic patients and healthy controls, but intima of uremic arteries was significantly thicker than that of controls. Ruengsakulrach et al. (13) reported that incidence of IH in the radial artery of 150 patients with advanced coronary artery disease was 94%, but that of atherosclerosis was only 5%. In this study, IH were observed in 74%, of 90 uremic patients, and atherosclerosis only in 2.2%. Although upper normal limit of radial artery in healthy persons measured by ultrasonographic examination is reported to 250 µm, there is no study demonstrating it by histologic examination. In this study, mean IMT in uremic patients was 430±132 µm (133-760 µm). Of the total 90 patients, 82 patients (91%) had increased IMT (more than 250 µm).
In this study, early AVF failure within 1 yr after the operation occurred in 31 (34%) of the total 90 patients. This incidence was similar to other reports (14-16). Mean radial artery IMT was thicker in failed group than in patents group (486±130 µm vs. 398±130 µm, p=0.004). The incidence of IH in the failed group was also higher than that in the patent group (43% vs. 9%, p=0.002). In order to evaluate the impact of IMT on the early AVF failure, we divided the total patients into two groups using threshold of 500 µm of IMT. Upper normal limit of the radial artery IMT in general population is known to be less than 250 µm (9, 17). Our study showed that 91% of uremic patients had IMT more than upper normal limit and mean IMT in total 90 patients was 430±132 µm. So we decided to cut off value 500 µm of IMT, which represents both double folds of upper normal limit and near level of sum of mean value of IMT and 1 standard deviation in the total patients. The AVF failure within 1 yr after the operation in the patients with IMT ≥500 µm was higher than that in the patients with <500 µm (72% vs. 50%, p=0.017).
There is no well-defined mechanism to explain how increased radial artery IMT causes early AVF failure. We suggest some possible mechanisms. First, increased IMT causes luminal narrowing and loss of vascular elasticity, which increases arterial stiffness. These two factors prevent to increase AVF blood flow. Second, increased IMT may include IH. It may directly extend to venous site and cause venous stenosis near the anastomosis site (3). Venous stenosis decreases AVF blood flow and directly induces AVF failure. In this study, patients with IMT ≥500 µm had higher incidence of IH, compared to patients with IMT <500 µm (92% vs. 32%). Low blood flow and small internal diameter of the radial artery is known to be risk factors of early failure of radiocephalic AVF. In previous study and this study, we investigate partial arterial specimen obtained from the incision site of AVF operation. So we focused only on arterial alteration such as IH and IMT and we did not evaluate arterial blood flow or internal diameter of the radial artery. Vein abnormalities such as small internal diameter or recent vein injury can cause early AVF failure (1, 18). In our hospital, when the cephalic vein was too small to create a radiocephalic AVF or it was collapsed because of recent multiple punctures, we did not place radiocephalic AVF. And in order to minimize the impact of vein injury, this study excluded the patients who had a history of central venous cannulation ipsilateral to the AVF surgical site.
Can radial artery biopsy performed during the operation influence on AVF patency? There is no data available to explain it at this moment. In this study, 10-mm long partial arterial walls were obtained from the incision sites of the radial arteries with elliptical form during the operation. There was no any complication of the biopsy. We previously reported that the early failure of the radiocephalic AVF operation without arterial biopsy occurred in 12 of the 58 patients (21%) within 4 months after the operation (8). In this study, the AVF failure developed in 18 of the 90 patients (20%) within the same period. So we do not think that the arterial biopsy influences on the AVF patency.
In this study, only age was an independent risk factor for increased radial artery IMT. Incidence of diabetes mellitus in the patients with IMT ≥500 µm was higher than that in the patients with IMT <500 µm. With multivariate analysis, diabetes mellitus tended to be a risk factor but it was not statistically significant. Our previous study and other studies showed that diabetes mellitus is an independent risk factor of IH (3, 13, 19, 20). But which diabetes mellitus is an independent risk factor of IMT or not has been reported yet. Future study is needed to evaluate the impact of diabetes mellitus on radial artery IMT.
In conclusion, our findings suggest that increased radial artery IMT is closely associated with early failure of radiocephalic AVF in HD patients. Therefore, if we can detect radial artery IMT in pre-dialysis uremic patients who will receive the AVF operation, it will be helpful for the surgeon to decide which the radial artery is adequate or not for the AVF operation. In contrast to IH, radial artery IMT can be easily measured by high-resolution ultrasonography before the operation. We recommend that ultrasonography should be performed in uremic patients, especially elderly and diabetic patients before the AVF operation and radiocephalic AVF operation should be avoided in patients with increased radial artery IMT.


 XML Download
XML Download