

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatitis B virus (HBV) persistently infects approximately 350 million people worldwide, and induces a spectrum of chronic liver disease ranging from chronic hepatitis through liver cirrhosis to hepatocellular carcinoma (HCC) (1). The persistent HBV carrier state is very frequently (up to 90%) transmitted from infected mothers seropositive for hepatitis B e antigen (HBeAg) to their babies (2, 3) and it used to be responsible for the majority of persistent HBV infections in Korea.
Presence of hepatitis B core antigen (HBcAg) in the hepatocyte is related to the presence of HBeAg as a marker of HBV replication, and usually connected with active inflammation of liver disease (4, 5). However, HBV replication is not always associated with hepatic damage. HBcAg has been detected in the hepatocyte nucleus and cytoplasm in various degrees (6, 7). The variability in these previous results may be related to differences in the clinical features, race, age, and region. An interesting issue raised is whether the degree of expression of HBcAg in the hepatocyte nucleus and cytoplasm reflects the level of viral replication and histological activity in the same age population with chronic HBV infection.
Two forms of chronic HBV infection are distinguished. One of them is characterized by the high level of viremia, hepatitis B e antigen (HBeAg) and absence of anti-HBe antibodies. Lack of HBeAg is usually connected with biochemically and histologically inactive disease as well as with the significant reduction of HBV replication, but up to 9% of such patients show active inflammatory process despite anti-HBe seroconversion (8, 9).
The aim of study was to evaluate the degree of HBcAg in the hepatocyte cytoplasm and nucleus and compare those results with histological activity of the disease as well as with serum HBV DNA level according to HBeAg status in the young patients with chronic B viral hepatitis.
MATERIALS AND METHODS
Patients and serological studies
One hundred-two patients (all men, mean age=19.7±1.4 yr old), who had been admitted to Wonkwang University Medical Center in Iksan, Korea between 1999 and 2003 and then diagnosed as seropositive for hepatitis B surface antigen (HBsAg) for more than 6 months, were selected. Patients with evidence of autoimmune hepatitis, Wilson's disease, primary biliary cirrhosis, anti-HCV positive, toxic and alcohol abusers were excluded. They had never received any antiviral or immune modulatory therapy. All patients gave informed consents for the liver biopsy procedure.
Laboratory assays
HBsAg, antibody against hepatitis surface antigen (anti-HBs), HBeAg, anti-HBe, anti-HCV, anti-HDV and anti-HIV were determined by enzyme immunoassay (Abbott Laboratories, Chicago, IL, U.S.A.). Serum HBV-DNA was assayed by a hybridization assay (Digene Hybrid Capture Assay, Digene Diagnostics, Gaithersburg, MD, U.S.A.). Lower and upper detection limits of the assay were 5 and 2,000 pg/mL, respectively. Levels of HBV DNA in sera were semiquantitively scored on a scale of 0 to 5, which were values corresponding to undetectable levels of <5, 6 to 50, 51 to 100, 101 to 150, 151 to 200, and >200 pg/mL, respectively.
Histological examination and immunohistochemical stains
All liver biopsies were done within one week of blood sampling. All were performed with Surecut needles (16G, TSK Laboratory, Japan). Liver biopsy specimens were fixed in 10% neutral-buffered formalin, embedded in paraffin. Sections were cut at 4 µm thick and stained with hematoxylin-eosin and Masson's trichrome. The liver histology was assessed by a pathologist who was blind as to the results of the liver biochemistry and HBV DNA levels.
The histological diagnosis of chronic hepatitis was made according to modified Histologic Activity Index (HAI) (11). The activity and the stage of chronic hepatitis were evaluated and graded from 0 to 4. The hepatitis activities of lobular activity and portal/periportal activity were classified into none, minimal, mild, moderate and severe grade. The stages of fibrosis were classified into no fibrosis, portal fibrosis, periportal fibrosis, and septal fibrosis, and cirrhosis.
Hepatocyte expression of HBcAg was studied by avidinbiotin immunoperoxidase method (rabbit anti-HBcAg from Zymed, San Francisco, CA, U.S.A.). The intracellular localization of HBcAg was labelled as cytoplasmic, nuclear or cytoplasmic plus nuclear by evaluation of at least 1,000 cells. Negative control experiments were carried out by substituting the primary antibody with phosphate-buffered saline. The degree of expression of HBcAg in the hepatocyte cytoplasm or nucleus was expressed as a proportion of the immunolabelled cells, as previously reported. A scale of 0 to 3, which were values corresponding to positivity in 0, 1 to 10, 11 to 50, and >50%, respectively, of hepatocytes examined, was used in our study.
Statistical analysis
Continuous variables with skewed distribution were compared by a nonparametric test, Mann-Whitney U test. Categorial data were tested by an χ2 test or Fisher's exact test. Correlation between different continuous variables with skewed distribution was tested by Spearman's rank correlation. Two tailed p value less than 0.05 was considered to be statistically significant.
RESULTS
Demographics
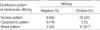
The demographics, liver biochemistry, and HBV DNA levels of all the patients are listed in Table 1. HBeAg-positive patients had a higher median HBV DNA level compared to HBeAg-negative patients (p=0.001). Among 27 patients without HBeAg, inactive carrier (ALT within normal range) was 15 (56%) and HBeAg negative hepatitis (increased ALT) was 12 (44%).
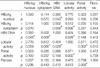
Sixty-nine of 75 (92.0%) patients with HBeAg and 16 of 27 (59%) patients without HBeAg had significant difference for intrahepatic HBcAg staining (p=0.000). The HBcAg staining pattern of 69 patients with HBeAg was as follows (Table 2): 20 nuclear (30%), 47 both nuclear and cytoplasmic (68%) and 2 cytoplasmic alone (2%). The HBcAg staining pattern of 16 patients without HBeAg was as follows: 9 nuclear (56%), 4 both nuclear and cytoplasmic (25%) and 3 cytoplasmic alone (19%). Patients with HBeAg had significantly higher expression of mixed pattern of nuclei of intrahepatic HBcAg than HBeAg-negative patients (p<0.001) (Table 2).
Relationship between the degree of expression of HBcAg in hepatocyte nucleus and cytoplasm with the histologic activity of liver disease
For HBeAg-positive patients, there was a highly significant correlation between the degrees of expression of HBcAg in the hepatocyte cytoplasm and lobular activities, and portal/periportal activities (Spearman rank correlation coefficient r=0.314, p=0.006 and r=0.283, p=0.01, respectively). There was no significant correlation between fibrosis and the degree of expression of HBcAg in the nucleus (r=0.023, p=0.84). On the other hand, there was a negative correlation between the degree of expression of HBcAg in the nucleus and lobular, and portal activities (r=-0.293, p=0.01 and r=-0.229, p=0.04, respectively) (Table 3).
For HBeAg-negative patients, the degrees of expression of HBcAg in the hepatocyte cytoplasm correlated positively with the lobular activities (r=0.512, p=0.006, respectively), but did not correlate with the portal activities and fibrosis. On the other hand, no significant correlation between the degrees of expression of HBcAg in the hepatocyte nucleus and histologic activities, and fibrosis was noted (Table 4).
Relationship between the level of HBV DNA in serum and the degrees of expression of HBcAg in the hepatocyte nucleus and cytoplasm
For HBeAg-positive patients, there was a highly significant correlation between the levels of HBV DNA in serum and the degree of expression of HBcAg in the nucleus (r=0.507, p=0.000). On the other hand, no significant correlation between the level of HBV DNA in serum and the degree of expression of HBcAg in the cytoplasm was noted (r=0.069, p>0.5).
For HBeAg-negative patients, there was a highly significant correlation between the levels of HBV DNA in serum and the degrees of expression of HBcAg in the nucleus and cytoplasm (r=0.392, p=0.043 and r=0.502, p=0.008, respectively).
Relationship between HBV DNA levels and with the histologic activity of liver disease
For HBeAg-positive patients, there were negative correlations between HBV DNA levels and histological activities (lobular activity and portal/periportal activity, p=0.05 and 0.02, respectively). For HBeAg-negative patients, HBV DNA levels positively correlated with lobular activity (p=0.028) while HBV DNA levels did not correlate with portal activity and fibrosis.
DISCUSSION
In the previous results, the expression pattern of HBcAg in hepatocytes was found to be related to the activity of liver disease in chronic HBV infection (11) especially when HBcAg was located in the cytoplasm of the hepatocyte (12). It also was found that nuclear but not cytoplasmic expression of HBcAg is associated with high HBV replication and low activity of liver disease in the chronic B viral infection (13). In this study, all these factors were assessed in the young age population which enabled us to compare the effects of these factors on the degree of HBcAg expression. The results suggested that only the extent of nuclear HBcAg expression correlated with HBV replication and also the extent of cytoplasmic HBcAg expression correlated with histological activity of liver disease in chronic HBV infection. The limitation of this study was that the HBV DNA levels were only measured at a single time point and most of patients had mild or moderate histologic activities of liver disease.
The interesting and significant finding was that there was a positive correlation between the histologic activity of liver disease and the degrees of expression of HBcAg in the hepatocyte cytoplasm in both HBeAg-positive and -negative patients. In the HBeAg-positive patients, there was a inverse correlation between the degree of expression of HBcAg in the hepatocyte nucleus and the histological activity of liver disease. This finding supported the importance of hepatocyte injury in determination of HBcAg expression pattern. To our knowledge, this could be the first study that the degree of expression of HBcAg in the hepatocyte cytoplasm as assayed by immunohistochemical techniques is helpful for estimating histological activity of liver disease in the young patients with chronic HBV infection. This inverse relation could suggest that the lysis of HBV infected hepatocytes was followed not only with the decreasing of serum viral load but also the degree of expression of HBcAg in the hepatocyte nucleus.
In 1987, Hsu et al. (7) showed that HBcAg was expressed at a relatively higher level on the nucleus than on the cytoplasm during the immune tolerance phase, in which there was little or no inflammatory activity in the liver, whereas expression of HBcAg in the nuclei decreased with a concomitant increase in the expression of HBcAg in cytoplasm during the immune clearance phase, in which there is active and ongoing hepatitis. Both studies postulated that expression of HBcAg on the cell membrane is the important event that triggers cytotoxic T cells with HBcAg receptors, resulting in lysis of HBV-infected hepatocytes. Viral peptides, rather than the whole viral antigen, are presented by the human lymphocytes antigen (HLA) class I molecules to the cytotoxic T cells in conjunction with adhesion molecules (14). The exact mechanism by which viral peptides are being incorporated into the HLA molecules was fully understood. The positive relationship between the degree of expression of HBcAg in the hepatocyte cytoplasm and histologic activity of liver disease supported that high level expression of HBcAg in the cytoplasm could reflect an increase in the availability of HBcAg for intracellular processing into the HLA molecules, and presentation as immune target to the cytotoxic T cells. In 1995, Chu et al. (12) denied the above-mentioned postulation and concluded that the cytoplasmic localization of HBcAg in patients with active hepatitis may be secondary to liver damage and regeneration.
In the present study, the interesting other finding was that there was a highly significant positive correlation between the levels of HBV DNA in serum and the degrees of expression of HBcAg in the hepatocyte nucleus, but there was no correlation between the degree of expression of HBcAg in the hepatocyte cytoplasm and the level of viral replication in the HBeAg-positive patients. Our result confirmed the relationship between nuclear HBcAg expression and viral replication. It has been shown that HBcAg was localized in the nucleus in quiescent cells but diminished in proliferating cells, and the replication of HBV was enhanced in quiescent cells but diminished in the proliferating cells (12). Expression of HBcAg in the hepatocyte nucleus was likely to be important in viral replication.
However, the mechanism for a significant correlation between the level of HBV DNA in serum and the degrees of expression of HBcAg in the hepatocyte nucleus rather than in the cytoplasm has remained unclear. HBcAg was a translational product of the pre-core/core gene of HBV and the carboxyl-terminal arginine-rich region of HBcAg has a nuclear localization signal (15). After entry into hepatocytes and transportation of the uncoated virus into the nucleus, viral DNA exists as a covalently closed circular (ccc) DNA, which serves as the template for transcription of pregenomic RNA (16). Some pregenomic RNAs was transported to the cytosol where formation of the viral nucleocapsid occurs along with the polymerase into core particles (17). Cytoplasmic core-packed viral DNA could also reenter the nucleus to amplify nuclear ccc DNA which in turn could provide more viral DNA for the production of new virions (18, 19). Our finding of a significant correlation between the degrees of HBcAg expression in the hepatocyte nucleus and the level of viral replication in chronic HBV infection supports this re-entry amplifying mechanism.
Though HBeAg seroconversion was commonly taken as a therapeutic endpoint in the past, increasing evidence showed that disease progression can continue in a significant portion of patients after HBeAg seroconversion, especially in the Asia and Mediterranean population (20, 21). We found that there was correlation between HBV DNA levels with lobular activity of liver disease in the HBeAg-negative which is in agreement with other previous studies (22, 23). This finding confirms that active viral replication is still present in a certain proportion of HBeAg-negative patients, and increased HBV DNA might be used as a marker to identify HBeAg-negative patients who have a higher risk of active liver disease. Some HBeAg-negative patients who have the inflammatory response and viral clearance might have precore mutation or/and core promoter mutations to escape immune clearance (24-27). In contrast, one reported that core promotor mutations were not associated with the enhanced viral replication (28). These mutations and unknown other factors may be related to the localization of HBcAg in the hepatocyte, therefore the virus might gradually replicate and develop inflammatory response in the liver. More studies are required to document whether core promotor mutations have any effects on the chronic hepatitis B disease.
Our study had limitations similar to those of other crosssectional studies (8, 13, 28). As hepatic inflammation may fluctuate with time, we can not be absolutely sure of the final outcome of these patients. This issue could only be satisfactorily addressed by a longitudinal study with paired liver biopsies.
In conclusion, the degrees of cytoplasmic HBcAg expression correlated with histological activity of liver and also the degrees of nuclear HBcAg expression correlated with HBV replication in the young patients with chronic HBV infection. These finding leads to the proposition that the nuclear localization of HBcAg may amplify ccc DNA in the replication period of HBV and cytoplasmic localization may induce interaction between T cell and infected hepatocyte.


 XML Download
XML Download