

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Kawasaki disease is an acute systemic vasculitis and its diagnosis is made on clinical features. Main complication of the disease is coronary artery lesion that may result in myocardial infarction or sudden death. Coronary artery aneurysms or ectasia develop in approximately 15-25% of untreated children (1). Since the intravenous immune globulin (IVIG) and aspirin therapy have been introduced, its mortality rate has decreased to 0.1%, but cardiac sequelae continues to occur in about 13% of Kawasaki disease patients (2).
The etiology of Kawasaki disease is largely unknown despite the various suggested hypotheses. Based on epidemiologic and clinical manifestations, it is thought that Kawasaki disease is caused by some infectious agents (3-10). Hypercytokinemia and hyperchemokinemia have also been observed and are thought to cause vascular injuries by inflammatory reaction and immunologic activation (11). Genetic factors are also thought to have influences on the development and progress of Kawasaki disease (12, 13). Up to present days, Kawasaki disease is thought to be an infectious disease manifested by immunologic reaction in genetically susceptable person.
Angiotensin converting enzyme (ACE) breaks down the potent vasodilator, bradykinin to its inactivate metabolite and catalyzes angiotensin I to angiotensin II. Angiotensin II promotes hyperplasia and hypertrophy of vascular smooth muscle cells, induces the production of proinflammatory cytokines and causes endothelial dysfunction by free radical generation. By playing an important role in cardiovascular regulatory system, ACE gene has been proposed to be associated with various cardiovascular diseases, such as ischemic heart disease, hypertrophic cardiomyopathy, idiopathic dilated cardiomyopathy, and vascular hypertrophy (14). Among the different ACE genetic loci, the insertion/deletion polymorphism coded within intron 16 has been studied in many literature to find the association with such diseases.
However, there has been few studies regarding the association between the polymorphism of ACE gene and Kawasaki disease. The present study investigates whether the I/D polymorphism of ACE gene (DD, ID, II) is associated with the prevalence and severity of Kawasaki disease among Korean pediatric populations.
MATERIALS AND METHODS
Study subjects
Fifty five Kawasaki patients (mean age 28.2±25.2 months) diagnosed at Ewha Womans University Mokdong Hospital from January 2001 to June 2003, and 43 healthy children (mean age 28.5±17.2 months) were enrolled. Kawasaki disease was diagnosed by its clinical features, that is fever lasting for at least 5 days, accompanied by 4 of the 5 classical signs: 1) bilateral bulbar conjunctival injection; 2) pharynx, injected and/or dry fissured lips, strawberry tongue; 3) changes of the peripheral extremities in the acute phase or periungal desquamation in the subacute phase; 4) nonvesicular rash; 5) cervical adenopathy, ≥1.5 cm. The diagnosis was made if he/she had typical manifestations even before less than 5 febrile days of illness. All patients were treated with immunoglobulin (2 g/kg) on the day of diagnosis. High dose (50 mg/kg/day) aspirin was given from the day of diagnosis and its dosage was changed to 5 mg/kg/day after 2 nonfebrile consecutive days.
Two dimensional echocardiography was done to evaluate cardiac complications. Coronary arterial lesion was defined as following: 1) inner diameter that is >3 mm in children <5 yrs old and >4 mm in children ≥5 yrs old; 2) internal diameter of a segment ≥1.5 times that of an adjacent segment; or 3) lumen with irregular surface. Among these patients, 17 showed coronary dilatations and 38 did not.
Informed consent was obtained from his/her parents prior to the participation in the study. The study was approved by the hospital's ethics commitee.
ACE genotyping
Each of the subjects' DNA was extracted from whole blood at the time of diagnosis using QIAamp DNA Blood Mini Kit (Gene Company LTD., Chai Wan, Hong Kong). DNA fragments were amplified through polymerase chain reaction (PCR), which was carried out in a total volume of 10 µL containing 50 ng of genomic DNA, 200 mM dNTPs, 0.3 mM/mL of each primers (5'-CTGGAGACCACTCCCATCCTTTCT); (5'-GATGTGGCCATCACATTCGTCAGAT) in PCR buffer with 0.5 units Taq DNA polymerase (Takara, Shiga, Japan). After the initial denaturation step (10 min at 95℃), 35 cycles were repeated for 30 sec at 94℃, 30 sec at 52℃, 90 sec at 72℃, and 5 min at 72℃. DNA fragments were then separated by electrophoresis on 2.5% agarose gel.
Statistical analysis
Student's t-test was used to compare the demographic characteristics between the two groups. Chi square test and Fisher exact test were performed to compare the genotype and allelic frequencies between the two groups. Its frequencies were compared by odds ratio. p value less than 0.05 was considered significant.
RESULTS
The mean age of Kawasaki group (28 boys and 27 girls) was 28.2±25.2 months, and that of the control group (30 boys and 13 girls) was 28.5±17.2 months. Among 55 Kawasaki disease patients, coronary dilatation was observed in 17 patients (8 boys and 9 girls, Table 1)
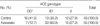
Frequencies of ACE genotypes (DD, ID, II) were 12.7%, 60.0%, 27.3% in Kawasaki group, and 41.9%, 30.2%, 27.9% in control group respectively, indicating low rate of DD genotype (p<0.01, odds ratio=0.2) and high rate of ID genotype (p<0.01, odds ratio=3.3) among Kawasaki patients (Table 2).
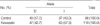
Comparing allelic (I, D) frequencies, I allele was more prevalent in Kawasaki group than in control group (57.3% vs. 43.0%, p<0.05, odds ratio=1.78, Table 3).
DISCUSSION
The ACE gene is localized on chromosome 17q23 and is characterized by a major insertion/deletion polymorphism consisting of the presence or absence of a 287-base pair Alu repeat sequence within intron 16 (15). Angiotensin converting enzyme is an ectoenzyme found on the external surface of the endothelial and epithelial cell membranes. It enhances the synthesis of angiotensin-II, that promotes proliferation, migration, and hypertrophy of vascular smooth muscle cells. Angiotensin II also induces the production of proinflammatory cytokines and matrix metalloproteinases (16, 17). Moreover, the increased free radical generation by angiotensin-II contributes to endothelial dysfunction (18, 19).
In humans, the ACE activity is partly under genetic control. It is suggested that about half of the interindividual difference in ACE levels may be accounted for its polymorphism (19, 20). It is reported that mean ACE levels were lowest for II homozygotes, highest for DD homozygotes, and intermediate for ID heterozygotes (18, 21). Danser et al. explained the higher ACE levels observed in subjects with D allele than those with the II genotype by the sequence harbored in the insert of ACE gene. This sequence was said to be very similar to a silencer element (22). But it is not clear whether increased levels of ACE actually affects the levels of angiotenisn II because the renin-angiotensin system is regulated by feedback mechanism (22).
Angiotensin converting enzyme is mainly produced by vascular endothelial cells (23). In Kawasaki disease, the associated endothelial cell damage subsequently lowers the ACE level. It is reported in some literature (24, 25) that serum ACE levels are significantly attenuated during the acute phase, and recovered during the convalescent phase of Kawasaki disease.
Slowik et al. (26) reported that the II genotype of ACE gene contributes to vascular dilatation at the site of aneurysm by 1) increased bradykinin activity, 2) another polymorphism responsible for vascular dilatation that is in linkage disequilibrium with ACE I/D polymorphism, 3) degeneration of endothelial cells, or 4) lack of vascular remodeling.
There is pathological difference between adult coronary artery disease (CAD) and that caused by Kawasaki disease. CAD caused by Kawasaki disease is characterized by vascular intimal thickening, whereas the adult CAD is characterized by atherosclerotic lesions initiated by atheroma and plaque formation. Thus, the pathophysiologic mechanism of myocardial ischemic development is also different; in adult CAD, plaque rupture and thrombus formation plays the important role, whereas in Kawasaki disease, coronary arterial narrowing by intimal hyperplasia is responsible (24).
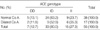
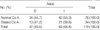
In this study, the ID genotype was more prevalent (59.3 vs. 30.2%, p<0.01), and the DD genotype (12.9 vs. 41.9%, p<0.01) was less prevalent in Kawasaki group than in control group. And I allele was more prevalent in Kawasaki group than in control group. However, both genotype (DD, ID, II) and allelic frequencies were not statistically different between Kawasaki disease patients with coronary dilatations and those without. Therefore, ACE gene I/D polymorphism was thought to be associated with the prevalence of Kawasaki disease but not with the development of coronary lesions. These results are similar to the report by Wu et al. (13) that the DD genotype was present in lower frequency among Kawasaki patients and ACE polymorphism was not associated with coronary aneurysmal formation. These results are different from the study by Takeuchi et al. (27) that the II genotype of ACE gene is more prevalent in Kawasaki disease and those with coronary aneurysm. These inconsistent results may be accounted for different ethnic traits of the individual population.
In conclusion, the ID genotype is present in a significantly higher frequency and DD in lower frequency among Kawasaki disease patients than in control subjects. In addition, there are no significant association between ACE I/D polymorphism and the coronary artery aneurysm formation in Kawasaki disease patients. Because the study groups are relatively small size in number, it is difficult to generalize these results. In this study, the coronary arterial dilatation was observed in 17 out of 55 Kawasaki patients. This is higher than that in previously reported literature. It can be accounted for either 1) longer duration from the onset of illness to the infusion of immunoglobulin, 2) other factors that may affect the development of coronary arterial lesions in Kawasaki disease, such as different ethinicity or 3) selection bias caused by limited number of enrolled institution and small number of patients. IVIG is recommended to be given within the first 10 days of illness and, if possible, within 7 days of illness. Since the duration of febrile days before the diagnosis and the IVIG infusion were 4.6±1.6 days (range, 2-8 days) in our study groups, the first explanation seems less likely.
Further study is required to clarity the association.

 XML Download
XML Download