

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asthma is a chronic inflammatory disorder of the airways characterized by bronchial hyperresponsiveness, reversible airflow limitation, and respiratory symptoms (1, 2). Internationally, the prevalence of asthma has increased over the last 3 decades (3-5), and in the Asia-Pacific region asthma causes considerable morbidity, with 15% of teenagers troubled by exercise-induced symptoms during the past 12 months (6). Furthermore, asthma mortality rates in more affluent areas, such as Hong Kong and Japan, are similar to those reported in Western countries (6). Studies in Korea also bear witness to these increasing trends (7, 8). The reported prevalence of asthma in Korea ranges from 2 to 13% (9-18). However, its prevalence in the elderly has been reported to be very high, at 12.7% in those aged 65 or more (15). Indeed, with a population estimated at more than 48 million, and a life expectancy of 72.0 yr for males and 79.5 yr for females (19), Korea faces an important public health challenge in terms of dealing with chronic diseases such as asthma.
In addition to its increasing prevalence, the economic impact of asthma is also substantial and continues to grow. The total cost of the disease in the United States was estimated to be U$4.5 billion in the mid-1980s, whereas in the first half of the 1990s, this estimate had increased to between U$6.2 and U$10.7 billion (20-22). In Korea, where health insurance is mandatory and the cost of medical care is only covered in part by health insurance, the importance of economic outcomes also continues to grow although little data is currently available.
The purpose of this review is to present an overview of the current disease status with respect to the prevalence, mortality rate, socioeconomic burden, quality of life and the treatment patterns of asthma in Korea, to identify barriers to improvements in asthma care and to provide recommendations for action at the national, organizational and individual levels. For this, all relevant English and Korean language articles were retrieved using PubMed (www.ncbi.nlm.nih.gov/entrez/query.fcgi) and KoreaMed (www.koreamed.com) from November 2004 to January 2005. Results were limited to the articles published between 1990 and 2004. In addition, various online resources through internet search engines were used.
PREVALENCE AND ASSOCIATED RISK FACTORS
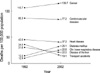
Recently, several large-scale studies of different population in Korea (9-17) have reported asthma prevalence ranging from 2 to 13% (Table 1). These differences are probably ascribable to different case definitions, methodologies, and a tendency to survey children rather than adults due to the relative ease of implementing studies in a school environment. According to the latest summary issued by the global burden of asthma by the Global Initiative for Asthma (GINA) program, the prevalence of clinical asthma in Korea is estimated to be 3.9% (23). The prevalence of asthma tended to be higher in children than in adults and was found to depend significantly on their place of residence, for example, it was found to be higher in Seoul than in provincial cities (7). According to 1998 data (11), childhood asthma was less prevalent in Korea than in other developed countries. However, among the elderly (aged 65 yr or older), its prevalence was found to be high at 12.7% in 2001 (15), which is about three times higher than among English or US elderly (24, 25). Although estimations of asthma prevalence in older age groups differ greatly between countries because of overlapping diagnoses, and poor patient perception of symptoms (24), this rate is unexpectedly high. In the elderly, asthma is an important problem because it is usually underdiagnosed and hence inadequately treated (24-26). Interestingly, Korean adults and children appear to have a later average age of asthma onset than other Asian populations (12) (Fig. 1). This is likely to be due to the underdiagnosis of early stage asthma by general physicians. Some investigators have reported that an underdiagnosis rate by general physicians was 21% (27). Another contributable factor may be that a high proportion of Korean people, at least initially, turn to traditional medicine for medical help (28-30), which delays the diagnosis until they are referred to hospitals or emergency department with severe symptoms. Finally, racial differences may be a consideration.
Age, sex, affluence, genetic predisposition, climate, outdoor air quality and cigarette smoking have all been found to be associated with asthma (7, 12, 15, 31-33). Studies suggest a higher incidence of asthma in children than in adults (9-15, 17, 34), and male asthmatic patients were found to be more often hospitalized or treated at a tertiary medical centers than their female counterparts (34, 35). In a regression analysis of the Asthma Insights and Reality in Asia-Pacific (AIRIAP) data for the eight areas of Asia-Pacific countries including Korea, it was found that a low household income is significantly associated with the likelihood of having moderate or severe persistent asthma symptoms (p=0.002 compared with a high income status) (12).
It has been reported that the genetic variations of the chemokine (C-X-C motif) receptor 3 (CXCR3) (36), the signal transducer and activator of transcription 4 (STAT4) (37), a disintegrin and metalloprotease 33 (ADAM33) (38), and Tumor necrosis factor-alpha (TNF-α) (39) are associated with the susceptibilities to the development of asthma and its intermediate phenotypes in the Korean population. The IL-4 cytokine gene cluster and/or the T cell receptor α/δ gene complex are believed to be associated with the expression of bronchial responsiveness to methacholone in nuclear families (40), and a polymorphism in exon 7 of chromosome 11q13 was found to be significantly associated with histamine release from basophile to anti-IgE stimuli in 80 randomly recruited asthmatic children (41). Specific environmental allergens also play important roles in asthma development in Koreans. Spider mites (Citrus red mite) (42, 43), the European red mite (Panonychus ulmi), (44) and the two-spotted spider mite (Tetranychus urtcae) (44), have been identified as important allergens in the development of work-related asthma and rhinitis symptoms and toluene diisocyanate has been most commonly implicated allergen in occupational asthma in Korea (45). A number of studies have documented an association between air pollution and asthma-related morbidity in Korean cities and have linked active smoking with asthma prevalence and severity (15, 28, 29, 46-48).
MORTALITY
The accurate determination of the asthma mortality in Korea is difficult. Because large-scale medical databases tend to group asthma data along with those of other disease states, or to group it with less specific group diagnoses such as 'Chronic lower respiratory diseases' (49). According to the Korea National Statistical Office data, the death rate from chronic lower respiratory diseases (including asthma) between 1992 and 2002 increased from 12.9 to 22.6 deaths per 100,000 of the population (50). In 1992, chronic lower respiratory diseases were ranked as the eighth leading cause of death in Korea, and in 2002, this had risen to fifth place proceeded only by diabetes mellitus, heart disease, cerebrovascular disease, and cancer (50) (Fig. 2). According to the latest GINA estimates, there are 4.9 asthma related deaths per 100,000 asthmatics each year in Korea (23). Globally, respiratory diseases are responsible for 6.3% of all death and asthma for 0.4% (51). Several risk factors of asthma mortality have been identified in the Korean population. These include cigarette smoking, chronic asthma severity, frequent hospitalization, the duration of recent asthma exacerbations, age and a female sex (28, 52, 53).
COST OF ILLNESS
At present, little data is available on the economic burden posed by asthma in Korea. However, indirect estimates may be made based on the market shares of asthma medications in Korea. According to the data from the pharmaceutical industry (54), from 2001 to 2004, the annual gross value of drugs sold in Korea increased by nearly 50% (from U$3.48 to U$5.21 billion) and the proportion shared by drugs for asthma treatment in respiratory drug market increased by approximately 36% (from U$51.8 to U$70.6 million). Research in this area is underway, with a large-scale analysis being performed using data from Health Insurance Review Agency (HIRA), the 1998 National Survey on Health and Nutrition in Korea, and an ongoing patient survey. Results are expected to be published soon.
QUALITY OF LIFE
To adequately account for cultural and behavioral factors, a quality of life questionnaire for adult Korean asthmatics (QLQAKA) was developed (55), and in a multicenter study 5 using QLQAKS, it was found that dyspnea (87%), difficulty in sputum discharge or throat clearing (87%), strenuous activity limitation (84%), and coughing (82.4%) were most frequently complained about by adult asthmatics (55). The AIRIAP study revealed that approximately one-third of all Korean asthmatic patients felt restricted in terms of their abilities to perform the routine activities of daily living such as, exercise, social activities, or sleeping (12). This survey also reported that 52% of asthmatic patients had experienced daytime symptoms during 4 weeks prior to completing the questionnaires, and that 41% of patients with asthma had been woken at night by their symptoms (12). Another study conducted to assess the quality of life of 189 patients showed that running, walking, and hurried movements appeared to be the most impaired daily activities (56). The characteristics that significantly impaired an individual's quality of life score were disease severity, level of asthma control and symptom attacks during the previous 3 months (all p<0.001) (56). Interestingly, a discrepancy was identified between perceived and actual asthma control in a substantial number of asthma patients. According to AIRIAP data, about one-fifth of Korean asthmatic patients with severe persistent symptoms considered that their asthma was adequately controlled, despite their current symptoms suggesting otherwise (12) (Fig. 3). This is due in part to the fact that some asthmatics have poor symptom perception (57-59) and partly because asthmatics in Korea are not adequately educated about the practical and theoretical aspects of asthma management (60, 61).
TREATMENT PATTERNS
No national guidelines concerning best management practice of asthma have been issued in Korea, although three academic associations have published separate guidelines (62-64). However, almost half of the physicians (43%) in 325 Korean clinics surveyed by the HIRA either did not use or were unfamiliar with these guidelines (65). Therefore, few asthma patients used or were prescribed inhaled corticosteroid by their physicians to prevent symptoms (65) (Fig. 4). The reasons for this reluctance to prescribing inhaled corticosteroid as cited by physicians in the HIRA survey were, in decreasing order; lack of patient education concerning inhaler use, high cost, patient refusal to use, and side effects (65). In addition, according to the AIRIAP survey, 65% of patients with asthma in Korea have never undergone a lung function test, and only 32% of patients reported that they had undergone a lung function test during the previous year (12). Moreover, although 6% of patients owned a peak flow meter for self-monitoring, only 20% of them used it daily, whereas another 20% used it on a symptomatic basis (12). Another survey found that patients who used a nebulizer at home were not properly instructed as to how to use it, and did not follow equipment maintenance procedures (66). However, paradoxically, most Korean asthmatics were satisfied with their treatment, although many expressed a need for more information on the disease (12). This 'disconnect' from the guidelines by physicians has had a major impact on the management of asthma patients. To reduce this gap, an 'Easy Asthma Management' study is currently underway in Korea. The purpose of this study may provide a simple stereotyped algorithm using a computer based program to allow clinicians to easily diagnose asthma and implement its correct management.
In December 2004, it was estimated that 11.9 million Koreans had access to the World Wide Web (WWW) and the number of allocated IP addresses allocated in Korea ranked eighth worldwide (67). Nowadays, computer-based educational programs available on the WWW are believed to be an effective alternative as they overcome the cost and time barriers that prevent implementation of education programs for asthmatics (68). However studies have shown that asthma educational material on the web sites is highly variable in quality and content, lacks detail of the core concepts essential for asthma education, and fails to meet patients needs (69, 70).
SUMMARY
This review showed that the prevalence of asthma in Korea ranges from 2 to 13%, and that physicians and patients often underestimate its severity. Mortality from chronic lower respiratory diseases including asthma increased from 12.9 to 22.6 deaths per 100,000 of the population between 1992 and 2002. Disease severity, level of control, and symptom state were all found to negatively impact the quality of life of asthmatics. Moreover, although international and Korean asthma management guidelines are available, primary care physicians are largely unfamiliar with or fail to implement them.




 XML Download
XML Download