

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Extended life span has changed the pattern of disease prevalence. Unlike other diseases whose incidences have been diminished, the incidence of spinal pain has been increased (1, 2). Moreover, its onset is more attributable to degenerative changes than to traumatic lesions. The treatment for spinal pain is now pursued on higher demand. Accordingly, recent extensive researches have been focused on the degenerative spinal pain syndromes, yet mostly on the lumbar spine (3-6). Meanwhile, cervical degenerative disorders have attracted little attention despite the increased prevalence of chronic neck and arm pain or cervicobrachialgia, along with the increased prevalence of degenerative spinal diseases. Recently, cervical zygapophyseal joint is highlighted as a possible source of chronic neck pain and referred pain in the upper arm (7-9). In particular, the zygapophyseal joints are identified to be related with chronic neck pain in 54% of the patients after whiplash injury (10).
Since radiofrequency (RF) neurotomy has been suggested by Schaerer in 1978 to treat the neck pain, sporadic reports have been reported (11-14). However, these study results vary with respect to selection criteria, techniques used, and outcomes achieved (8, 9). Not all studies have selected patients on the basis of diagnostic blocks of cervical medial branches; or when used, such blocks were not controlled and the surgical techniques did not accurately target the cervical medial branches. These factors may explain why the reported results were not so encouraging in terms of proportions of patients relieved and the degrees of relief they obtained. However, a randomized controlled study and long-term follow-up is making RF procedure for cervicobrachialgia to be one of the promising techniques with anatomical accuracy of targeting the cervical medial branches (9, 14).
The present study was designed to assess the efficacy of comparative diagnostic blocks correlating with the outcome of RF neurotomies and to determine a better strategy to achieve improved outcomes in the patients with chronic cervicobrachialgia.
MATERIALS AND METHODS
Patient population
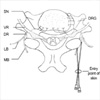
Between October 2003 and October 2004, a total of 28 patients underwent RF neurotomies for their cervicobrachialgia in our institution. Patients, who had chronic neck pain with or without referred arm pain more than 3 months, whose pain intensity was greater than 5 in visuoanalogue score (VAS), and whose primary source of pain was confirmed to be cervical zygapophyseal joints by comparative diagnostic blocks, were indicated for RF neurotomies. Thorough clinical and neurological examinations were conducted and simple radiographies were routinely performed. We paid special attention to pain-provocation and its radiation to the corresponding distribution of pain complaints by the light pressure on the cervical zygapophyseal joints, while pain responses were evaluated with the assumed level of cervical zygapophyseal joint arthropathies. All patients were interviewed by a pain-specialized nurse, who recorded pain distribution pattern, nature of pain, pain-related dynamic factors, and factors influencing the life pattern and daily activities. Pain distribution patterns were divided into type A, B, and C (Fig. 1); Type A indicates the pain distribution in the lower neck; Type B demonstrates the pain in the neck and shoulder; Type C with the pain in lower neck, shoulder, sometimes scapula, and upper arm. Excluded are the patients who had objective evidence of cervical radiculopathy with signs of myotomal weakness, sensory disturbances, and loss of reflexes. Patients who had collagen, vascular, or rheumatologic diseases were also excluded.
Preoperative diagnostic block
All patients had diagnostic blocks in the operating room under C-arm intensifier. To decrease the false positive rate, diagnostic blocks were performed more than twice in each patient. Targets of diagnostic blocks were determined mostly by pain distribution patterns. C4, C5, and C6 medial branches were chosen for type A and B pain distribution, and C7 was additionally included for type C. If patients showed pains on inner scapular area, medial branch of T1 was included. If patients showed bilateral pain distribution, targets were determined in both sides. Comparative blocks were performed in all the patients. Those who responded to first block and began to have similar degree of pain again were encouraged to have second block after at least one week. Those whose pain were not relieved by first block went on to other investigations. Those whose pain was markedly improved were not included in this study.
Nerve blocks were performed in a group (e.g., C4, 5, 6 and 7 together) rather than a single trial. Targets for C4, C5, and C6 were the centroid of the articular pillar. Target for C7 was supero-lateral aspect of C7 transverse process (Fig. 2). Target for C8 was supero-lateral aspect of T1 transverse process. After introducing the needle at the targets, and contrast dye was injected to confirm that dye is not drained into the vascular space. If the needle was confirmed to be placed in the target on slightly oblique view, 0.5 mL of 0.5% bupivacaine or 4% lidocaine was used for the first block. As for second block, local anesthetic agent which was not used for their first block were used. After injecting local anesthetics, patients were instructed to mark the changes in their usual pain in ''pain evaluation sheet'' as complete relief, nearly complete relief, 50% reduction of pain, slight reduction of pain, and no change every 1 hr except sleeping time for 3 days. If the patients demonstrated concordant pain relief greater than '50% of pain reduction' on comparative blocks, they were considered the candidates for RF neurotomies.
RF neurotomies
Only patients who began to experience the return of symptoms after second block returned to RF procedure. If patients' pain was markedly relieved by provocative blocks, they were discouraged to undergo RF procedures.
RF neurotomies were performed in an aseptic manner in the operating room. Patients were placed prone on the table with electrocardiography and blood pressure monitoring. C-arm fluoroscopic unit (OEC, U.S.A or Madison, Korea) was used to visualize the targets. To localize the ''pathological branches'', which are responsible for pain generation, the sensory-stimulation method was adopted. All cervical medial branches included in the diagnostic blocks were subject to sensory stimulation using lesion generator (Leibinger N50, Germany). Twenty one gauge of RF cannula of 100 mm long with 5 mm active tip (Precision Medical Engineering, U.S.A.) was used. RF cannula was advanced parallel to the plane of zygapophyseal joint in C4 - 6 medial branches to locate the needle in the center of waist of articular pillar. Using 50 Hz frequency of stimulation with 1 msec duration, stimulation on every medial branch was performed to locate the pathological branches. Stimulations elicited tingling sensation, electrical pain, or feeling of heaviness. If pain response was same as that of usual pain with stimulation lower than 0.6 V, the cannula was maintained for RF coagulation of the branches. In addition, absence of motor fasciculations in corresponding upper extremities was confirmed with 2 V at 2 Hz stimulation. RF neurotomies were performed upon confirming the pathological branches. After introduction of 1 mL of 2% lidocaine, RF electrode was inserted through RF cannula. Two targets were selected along the course of medial branch for lesioning (Fig. 3). First target was branch on the curving point of waist of the articular pillar on posterior-anterior projection. The second lesion was made after introducing the cannula deeper in the centroid of the second target in the articular pillar on lateral view. To avoid the escape of medial branches from extent of coagulation, additional lesions were made above and below the targets. RF lesion was created on medial branches at 80℃ for 90 sec. After RF Lesioning, 1 mL of mixture of 0.5% bupivacaine and 8 mg/mL of triamcinolone was injected on the lesioned area to decrease postoperative pain and neuritis.
Follow-up evaluation and surgical results
Patients were followed up for a minimum of 6 months up to 12 months after RF neurotomies. Patient outcome was measured with VAS score at 1, 2, 3, 6, 9, and 12 months after the operations. Outcome was arbitrarily graded as a successful outcome (more than 75% improvement), moderate improvement (between 50 and 75% improvement), and failure (less than 50% improvement). Categorical variables were assessed and compared by using chi-square, Pearson correlation, and ANOVA by SPSS statistical software program.
RESULTS
Clinical characteristics
Table 1 summarizes the clinical characteristics. Patients consisted of 15 male (54%) and 13 female patients (46%). Age at the time of evaluation and surgery ranged from 36 to 83 yr (mean 54.4 yr). Duration of pain prior to surgery ranged from 3 months to 40 yr (mean 2.9 yr). Preoperative severity of pain ranged from 5 to 10 (mean 6.6) in VAS. Analysis of pain distribution pattern showed type A in 6 (21%), type B in 6 (21%), and type C in 16 (57%) (Fig. 1). Five patients had history of whiplash injuries, and one patient had penetrating injury in the neck. Twenty patients had unilateral pain (9 in right side and 11 in left side), while 8 patients had bilateral pain.
Preoperative provocative test
Controlled block was performed at least twice in all patients. The third test was required in two patients, because the result of the second block was questionable. Interval between first and second blocks was 16.5 days. Pain distribution pattern was not significantly correlated with the results of diagnostic blocks in the study. All patients obtained significant (≥50% at least) pain relief on each controlled block to be potential candidates for RF neurotomies. Meanwhile, C4-C6 levels were most commonly selected for the targets of diagnostic blocks. Four patients showed incongruent level of pain relief on two consecutive diagnostic blocks.
RF Neurotomies and surgical outcome
All patients underwent electrical stimulation on each medial branch. Average stimulation intensity was 0.45 V, ranging from 0.3 to 0.69, to elicit pain response in cervical medial branches. Average number of lesioning was 8 per patient. Number of RF-lesioned nerve branches was 6 per patient. Most common involvement of nerve branches was C4 (89%), followed by C5 (82%), C6 (75%), and C7 (43%).
Postoperative pain relief was relatively constant until 6 months once patients obtained improvement by RF procedures. However, one patient among 28 patients showed the recurrence with same pain distribution between 6 and 9 months, and three patients recurred between 9 and 12 months. However, their degree of recurrent pain were not same as preoperative level, 64% of postoperative pain relief, to justify repeating the procedure. Interestingly, 6 patients out of 28 patients showed only modest decrease (32% improvement) of VAS. Increased physical activity after decrease of pain might contribute to the additional decrease of VAS in these patients.
Nineteen patients (68%) reported successful outcome according to outcome criteria after 6 months of follow-up (p=0.001), and among them, eight patients (29%) reported complete (100%) relief of pain. Two patients reported failure. Five patients who showed incongruent level of pain relief on two consecutive diagnostic blocks had unsuccessful outcome. These outcomes were relatively maintained until 9 months. However, patients with failure category were increased due to recurrences of pain 12 months after the procedure. Outcome was not significantly influenced either by the side or level of operation.
Among five patients with whiplash injury, three obtained complete relief of pain. One patient had 60% of relief of pain of preoperative level, yet pain relief was enough not to repeat the procedure. One patient who had history of whiplash injury showed earlier recurrence of pain 3 months after RF procedures, despite successful outcome in early period. He was advised to repeat diagnostic procedure but refused to do so.
Postoperatively, patients showed side effects including muscle cramping pain and numbness which lasted one or two weeks in most cases, but no longer than four weeks. Taking analgesic drugs for several days was enough to control these postoperative side effects. No patients were admitted for intensive control of post-operative pain. Complications such as motor deficit, infection, neuropathic pains, were not encountered after the procedures in our series.
DISCUSSION
Neck and arm pain is one of the most common causes for a visit to the hospital. They are often ascribed to the diagnosis as cervical spondylosis, characterized by narrowing of the intervertebral foramina by cartilaginous or osteophytes bar and osteophytes stemming from the intervertebral disc and zygapophyseal joints, which cause the compression of spinal nerves, intrathecal fibrosis, and axonal degeneration (15, 16). These pathoanatomical changes provide clinical background for open decompression or widening of intervertebral foramina. However, most patients with neck pain correlate poorly with cervical spondylosis, and rarely demonstrate manifestations of radiculopathy and myelopathy. Cervical spondylosis may occur without manifestation of pain, and many patients with neck pain shows absolutely no signs of spondylosis (17, 18). In addition, the advent of high resolution magnetic resonance imaging (MRI) enabled us to detect the disk herniation or cervical spondylosis more frequently than we used to do before. Nonetheless, abnormal findings on MRI often do not correlate with the symptoms of patients (19). On the other hand, prevalence studies revealed that actual prevalence of zygapophyseal joint pain could be as high as 63% among the patients with neck pain (7, 20). This strongly suggests that substantial number of patients with neck pain, whether combined with arm pain or not, are associated with zygapophyseal joint pain, unless neurological signs of radiculopathy or myelopathy are present. This was considered in this study as a guideline to select the patients as candidates for RF neurotomies to treat the patients with incapacitating neck pain with upper arm pain.
Pain distribution pattern was not as useful as that in lumbar zygapophyseal joint pattern in terms of determining the targets of diagnostic blocks. However, our classification was still useful to determine the level of blocks of medial branches. Type A indicates the pain distribution in upper level excluding the C7 or C8 levels. Therefore, it is likely to choose C4, C5, and C6 medial branches as targets for patients with type A. On the contrary, we included C7 or sometimes C8 for medial branch block in patients who showed pain distribution of Type C. Cervical medial branch blocks were favored in the patients with cervicobrachialgia unless they showed symptoms of radiculopathy, because this procedure is simpler, easier, and more convincing in identifying the painful zygapophyseal joints. All patients had more than twice of blocks in order to exclude the patients who showed the false positive responses. It is reported that single, uncontrolled blocks are compromised by a false positive rate of 27% in cervical zygapophyseal joint blocks (21). We selected patients for RF neurotomies if they showed more than 50% of pain relief after medial branch blocks. In addition, we later found that concordance of degree of pain relief between two consecutive medial branch blocks was also important to improve the outcomes. Four patients who showed incongruence between the two tests had failed to achieve good results after RF neurotomies in our series.
Once patients showed concordant responses to controlled diagnostic blocks, there has not been any failure to identify the 'pathological branches', presumed to be responsible for pain generation with electrical stimulation of low amplitude in all patients. Thus, we considered that a physiological approach to delineate the sources of spinal pain is crucial to successfully conduct RF neurotomies. As modern neuroimaging techniques, particularly MRI, CT, and CT-myelography, have been enhanced, the diagnosis of spinal pain became easier to perform, and surgical treatment is invited more frequently by developing better surgical methods and intraspinal fixing devices. Still, there is skepticism about the biased use of imaging techniques, which undermines the fact that spinal pain integrates physiological and pharmacological phenomena just like other pains (19, 22). These imaging techniques often do not contribute to the accuracy of diagnosis in the patients with cervical spondylosis. Therefore, we did not merely depend on modern neuroimaging techniques to identify the candidates for RF procedures unless they showed the symptoms and signs of radiculopathy or myelopathy. We believe that pain is a physiological manifestation which can not be often correlated with the anatomical derangement. Rather, physiological approaches, including pain mapping and nerve block, are more specific for diagnosing the source of pain in the patients with degenerative spinal pains.
Interestingly, we have five patients who had history of whiplash in our series. Their neck pains were not clearly diagnosed clinically or radiographically, yet they were identified by using the provocative techniques to block the painful zygapophyseal joints. It is reported that about half of patients with whiplash injury develop chronic neck pain, and its pain originates from the cervical zygapophyseal joints (10). Conventionally, chronic neck pain after whiplash injury defies any diagnostic techniques and treatments. This notion was mostly based on the reports of Quebeck Task Force on Whiplash-Associated Disorders, which emphasized that there were almost no literatures to validate the diagnosis and treatments for this condition (23). It is not infrequent to refer the patients consistently complaining neck pain to psychiatric consultation. The investigation of whiplash injuries has been mostly dependent on the clinical findings, plain radiograph, CT, and MRI. However, none of these methods has been successful to explain the exact pathology of neck pain. The most reasonable approach to investigate neck pain after whiplash injury is to provoke or eliminate the pain by stimulating or blocking the nervous structures presumed to be responsible for pain generation. Local anesthetic blocks of either the cervical zygapophyseal joint or medial branch have been developed to identify the source of pain. Application of these techniques to a large cohort of patients, many of whom had sustained whiplash injuries, revealed that between 25% and 62% were cervical zygapophyseal joint pain (24, 25).
Around 70% of the operated patients in our series showed a successful outcome after undergoing the procedures. Early reports claimed that between 50% and 90% of patients treated by RF neurotomies obtained at least 40% of relief of their pain, yet few studies reported complete relief (12-14). Their poor results can be explained by systemic review of their studies performed with vague criteria selection and inaccurate anatomical knowledge of the cervical medial branches. The surgical outcome was greatly improved after adopting the randomized, double-blinded, and placebo-controlled trials before RF procedures and using more accurate techniques to include the medial branches in the boundary of heating area (9, 26). Our results are not favorable compared with that of McDonald et al. (26). It is indeed hard to compare the results of these groups exactly. However, we have drawbacks of not being strict in selection of the candidates, because five patients did not show the congruence in terms of pain relief after diagnostic blocks. In addition, the number of RF lesionings was less, and we used RF cannula with smaller diameters in our series, compared with those of McDonald et al. series. These factors should be either eliminated or should be considered for changes to further enhance the efficacy of RF neurotomies in the patients with chronic cervicobrachialgia.



 XML Download
XML Download