

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In Korea, rapid socioeconomic growth has led to a more sedentary lifestyle and change in diet over the past several decades. As a result of prosperity, obesity has become an important health problem, as in some Western countries. While the prevalence of obesity in Asian populations is lower than that of Caucasian societies, the health risks associated with obesity have been reported to occur at a lower body mass index (BMI) (1).
Many studies have demonstrated a close relationship between body fat distribution and the occurrence of the metabolic syndrome; an excess of abdominal adipose tissue, especially intra-abdominal visceral fat, leads to obesity-related complications (2, 3). The area of visceral fat area is most accurately measured using computed tomography (CT). It is not practical, however, to measure the visceral fat area with CT in the clinic. Therefore, waist circumference (WC) is used as the best simple anthropometric index of abdominal visceral fat accumulation; these measures are related to cardiovascular risk in men and women (4, 5).
The Third Report of the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) discussed the importance of the metabolic syndrome, including waist circumference, as diagnostic criteria, in 2001 (6). However, the criteria were developed based on Western patients, therefore, generalization to Asian patients requires modification. In 2000, the WHO Asia-Pacific Region recommended abdominal obesity diagnostic criteria for Asian populations. Currently, NCEP ATP III criteria modified with the WHO Asia-Pacific Region waist circumference criteria are broadly utilized as diagnostic criteria for the metabolic syndrome in Korea.
However, among Asians, each ethnic group has their own anthropometric characteristics. Therefore, it is difficult to apply the same criteria to each of the different ethnic groups. Determination of accurate criteria for the diagnosis of 'obesity related disease' in Korean subjects is an urgent priority. Thus, the aim of this study was to determine the appropriate cut-off values, for visceral fat area and WC, that are associated with an increased risk for obesity-related disorder, and to validate diagnostic criteria for abdominal obesity and the metabolic syndrome in an adult Korean population.
MATERIALS AND METHODS
Subjects
Our study included 413 Koreans aged 18-70 yr (174 men and 239 women) who visited the obesity clinic at St. Mary's Hospital and Kangnam St. Mary's Hospital from January 1999 to August 2005. All subjects had performed a CT. All participants provided informed consent. This study was approved by the institutional review board of the St. Mary's Hospital and Kangnam St. Mary's Hospital. Excluded from this study were individuals with an identified secondary cause of obesity, pregnant or lactating women and patients with evidence of severe hepatic or renal disease. All individuals were evaluated by a physician, including a medical history and physical examination.
Anthropometric measurements
Anthropometric measurements were taken with subjects in light clothing and without shoes. Height and weight were measured using an automatic height-weight scale, to the nearest 0.1 cm and 0.1 kg. BMI was calculated by dividing weight (kg) by height2 (m2).
Waist and hip circumference were measured with a nonelastic tape measure. WC was measured at the end of normal expiration, at the midpoint between the lower border of the rib cage and the iliac crest. For the hip circumference, the tape was positioned around the hips at the level of the symphysis pubis and the greatest gluteal protuberance. Body fat percent was measured by bioimpedence analysis (Inbody 2.0, Biospace, Seoul, Korea); same equipment was used in both participating hospitals. Technicians were educated to provide precise anthropometric measurements according to guidelines used to reduce interpersonal variation.
Visceral and subcutaneous fat area
Cross-sectional abdominal visceral and subcutaneous fat areas were measured by computed tomography (Somatom plus, Siemens, Germany) using an established protocol (7). The same protocol was used at both participating hospitals. A cross-sectional scan at 10 mm thickness centered at the L4-L5 vertebral disc space, with the subject in the supine position, was obtained using a radiograph of the skeleton as a reference to establish the position of the scans to the nearest millimeter. Subcutaneous and visceral fat area (SFA and VFA) boundaries were defined using a manual cursor by delineating these areas with a graph pen. The adipose tissue areas were calculated by computing the fat area surfaces with an attenuation range of -190 to -30 Hounsfield units. The abdominal VFA was measured by drawing a line in the muscle wall surrounding the abdominal cavity. The SFA was calculated by subtracting the VFA from the total fat area (TFA). Then the VFA to SFA ratio (VSR) was calculated.
Metabolic variables
Blood pressure was measured with a mercury sphygmomanometer after 10 min of rest in the sitting position. Study subjects refrained from smoking or ingesting caffeine during the 30 min preceding the measurement. Cuff size was selected according to the arm circumference of the participants. The first appearance of sound (phase 1 Korotkoff sound) was used to define systolic blood pressure and the disappearance of sound (phase 5 Korotkoff sound) to define diastolic blood pressure (8). Two readings each for the systolic and diastolic blood pressure were recorded, and the average of each measurement was used in the final analysis. If the first two measurements were different by more than 5 mmHg, additional readings were obtained.
Blood samples were obtained in the morning after 12 hr of overnight fasting from an antecubital vein, and stored in vacutainer tubes containing EDTA and subsequently analyzed at a central laboratory. Fasting plasma glucose (FPG) was measured by the glucose oxidase method, and the total cholesterol (TC) and triglyceride (TG) levels by enzymatic procedures using an autoanalyzer (Hitachi 736-20, 7170 automatic analyzer, Tokyo, Japan). The high density lipoprotein (HDL) fraction was obtained after precipitation of apo-B containing lipoproteins with MnCl2.
Obesity-related disorders
Three obesity-related disorders were defined: hypertension was defined by use of antihypertensive medication or a systolic blood pressure ≥140 mmHg or a diastolic blood pressure ≥90 mmHg; hyperglycemia, was defined by use of antidiabetic medication or a FPG ≥110 mg/dL; and dyslipidemia, was defined by a TC ≥220 mg/dL or TG ≥150 mg/dL or HDL <40 mg/dL) (9).
Criteria for the metabolic syndrome
The metabolic syndrome was defined according to the 2001 NCEP ATP III (6), except for abdominal obesity determined by WC measurements which was not applicable to relatively lean Asians. According to the Asia-Pacific regional guidelines, abdominal obesity was defined as a WC >90 cm for men and >80 cm for women (1). The presence of the metabolic syndrome was determined by ≥3 of the following 5 parameters in patients: a WC >90 cm for men or >80 cm for women, serum triglyceride levels ≥150 mg/dL, serum HDL cholesterol levels <40 mg/dL for men or <50 mg/dL for women, systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg, and a fasting blood glucose ≥110 mg/dL.
In addition, individuals who reported currently using antihypertensive or antidiabetic medication were categorized as meeting the high blood pressure or glucose criteria, respectively.
Statistical analysis
The statistical analysis was performed using SPSS for Windows version 10.0 (SPSS Inc., Chicago, IL, U.S.A.). Data were expressed using gender-specific mean values and standard deviations for continuous variables. We used the independent sample t-test to examine the gender difference of continuous variables. The chi-square test was used to examine significance according to sex. Frequency of obesity-related disorder to BMI and VFA were calculated. In this study, high VFA was defined as more than 100 cm2 according to the Japanese visceral obesity criteria (9). The odds ratio for the metabolic syndrome according to VFA was calculated. To determine the cut-off values for VFA and WC, we examined the number of associated clinical diagnoses (ie, hypertension, hyperglycemia and dyslipidemia) at each VFA or WC level. The cut-off values of the VFA and WC associated with an increase in the prevalence of the obesity-related disorder was calculated using the receiver operating characteristics (ROC) curve. Next the sensitivity and specificity of each cut-off was estimated by identifying subjects with more than one clinical diagnosis. The cut-off value associated with the best combination of sensitivity and specificity was selected as the optimal threshold for each parameter.
A value of p<0.05 was considered to be statistically significant.
RESULTS
Characteristics of subjects
Characteristics of study subjects by gender are presented in Table 1. Of a total of 413 individuals, men (n=174) accounted for 42% of the subjects and women (n=239) did 58%. The mean BMI was 30.9±5.2 kg/m2 in men, and 29.9±5.7 kg/m2 in women. There was no significant difference between genders for BMI, waist/hip circumference ratio, total cholesterol and total abdominal fat area. However, the mean body fat was higher in women (38.5±7.0%) than in men (31.2±6.9%). Although the total area of abdominal fat was not significantly different, the VFA was higher for men (159.8±73.7 cm2) than women (127.4±58.7 cm2), and the subcutaneous fat area was higher in women (299.5±137.9 cm2) than in men (234.3±125.3 cm2). Therefore the VSR was higher for men (0.68±0.47) than for women (0.43±0.30) (p<0.001).
Prevalence of obesity-related disorder
For the prevalence of obesity-related disorders, hypertension was identified in 44.6% (n=184), hyperglycemia was 27.4% (n=113) and dyslipidemia was 58.1% (n=240) of participating subjects. The percentage of subjects, and the frequency of the 3 obesity-related disorders, in 4 subgroups determined by BMI (obese: BMI ≥25 kg/m2 and non-obese: BMI <25 kg/m2) and VFA (high VFA: VFA ≥100 cm2 and normal VFA <100 cm2) in consecutive subjects (167 men, 235 women) who underwent anthropometric measurements are shown in Table 2. The percentage of subjects who had no obesity-related disorder was significantly lower 16.7% (n=67), compared to one obesity-related disorder 42.0% (n=169) and two or more obesity-related disorders 41.3% (n=166). Consequently, the proportion of subjects with multiple risk factors was significantly higher in obese subjects with a high VFA. However, the proportion of non-obese subjects with a high VFA, and obese subjects with normal VFA was similar (Table 2).
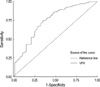
Cut-off values for visceral fat area and waist circumference associated with increase in the prevalence of the obesity-related disorders
The cut-off value for VFA using the ROC curve was 103.8 cm2 (sensitivity 74.5%, specificity 64.7%, p<0.001). Using the same method, the cut-off value for WC was 89.8 cm for men (sensitivity 84.7%, specificity 91.7%, p<0.005) and 86.1 cm for women (sensitivity 83.6%, specificity 62.9%, p<0.001) (Fig. 1, 2).
Prevalence of metabolic syndrome
The prevalence of the metabolic syndrome was 52.8% (n=218); men accounted for 62.1% (n=108) and women 46.0% (n=110). The odds ratios for the metabolic syndrome based on an increase in visceral fat compared to those within the reference range (VFA<100 cm2) were obtained. Each odds ratio showed a tendency to increase with VFA statistically (p<0.001) (Table 3).
DISCUSSION
An increased waist circumference has been demonstrated to be a good predictor of cardiovascular disease (5), and is an important diagnostic marker for the metabolic syndrome. Although CT scanning and magnetic resonance imaging are used for precise measurements of visceral fat (10, 11), simple anthropometric measurements for estimating the amount of visceral fat are essential for practical screening of the general population. On the basis of prior studies, the WC has been shown to directly reflect abdominal fat mass (12, 13).
WHO initially proposed a definition for metabolic syndrome in 1998 (14). The Third Report of NCEP ATP III proposed useful criteria for the diagnosis of the metabolic syndrome in 2001 (6). However, the measurements offered for cut-off criteria for abdominal circumference of more than 102 cm in men and more than 88 cm in women for abdominal obesity are based on Caucasian criteria. Therefore the prevalence of the metabolic syndrome, based on these criteria, in the Asian population is very low (15, 16).
A number of studies comparing Asian ethnics, such as Filipinos (17), Japanese (18) and South Asians (19) with Caucasians have reported that Asians had higher risk of diabetes and/or the metabolic syndrome even though they had lower fat measurements. Asian populations have been shown to have a higher body fat deposition at a lower BMI than Caucasians (20-22). Abdominal obesity promotes insulin resistance and leads to the metabolic syndrome (23). Therefore, at a relatively low BMI, Asians have higher glucose intolerance (24) and cardiovascular risk factors compared to Caucasians.
Accordingly, the criteria for obesity, as proposed by the Asian-Pacific region of WHO, is a BMI ≥25 kg/m2 (1). The cut-off values used for WC, to determine abdominal obesity, are 90 cm for men and 80 cm for women in Asian populations (1). According to these criteria, Kwon et al. (25) reported that the prevalence of the metabolic syndrome in the adult Korean population was 34.3% (men 26.3%, women 40.1%). Therefore, the metabolic syndrome is a serious problem in Korean society.
In 2002, a study on 1,193 Japanese subjects found that the WC measurement that equated with a VFA of 100 cm2 was a useful cut-off for the prediction of patients with more than one clinical diagnosis, i.e. dyslipidemia, hyperglycemia and hypertension. This 100 cm2 value is exceeded by 70% of those Japanese patients identified with coronary heart disease. Therefore, Japanese guidelines have established a cut-off point for waist circumference to be 85 cm in men and 90 cm in women (9).
However, in Korea, Choi et al. (26) and Park et al. (27) reported that the cut-off point should be a WC of 90 cm in men and 85 cm in women, and Lee et al. (28) reported that it should be 89 cm in men and 86 cm in women. Therefore, there remains controversy regarding the appropriate cut-off point for the WC as a diagnosis for abdominal obesity in the adult Korean population.
In our study, the cut-off value for VFA, that is associated with an increase risk for an obesity-related disorder using the ROC curve, was 103.8 cm2 (sensitivity 74.5%, specificity 64.7%, p<0.001). This cut-off point is similar to that used by the Japanese, 100 cm2 (13). The cut-off value for WC was 89.8 cm in men (sensitivity 84.7%, specificity 91.7%, p<0.005) and 86.1 cm in women (sensitivity 83.6%, specificity 62.9%, p<0.001). Our study results show a higher WC level in women than that offered by the 2000 WHO Asia-Pacific guideline, 80 cm (1), and many other studies in Korea agree that the cut-off value of 80 cm in Korean women is too low (25-28).
Our study had the following limitations. Because we recruited subjects from a specialty clinic, the findings from our study group cannot be generalized to the general Korean population. In addition, we had limited information on other, potentially important information such as smoking habits, alcohol use and whether subjects exercised. Moreover, the number of study subjects was small.
Further studies are necessary to define the level of abdominal obesity to predict cardiovascular risk among relatively lean Asians, and to unravel determinants of the metabolic syndrome for primary prevention. We would like to recommend that a standard health examination include assessment for the metabolic syndrome including abdominal obesity measurements, and based on the results secondary prevention be implemented immediately.




 XML Download
XML Download