

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Interleukin-10 (IL-10) is a multifunctional cytokine with diverse effects on the immune response. IL-10 limits inflammation and modulates immune response by inhibiting the production of various pro-inflammatory and Th1 cytokines and blocking the expression of MHC class II and co-stimulatory molecules on the surface of antigen presenting cells and promoting the development of regulatory T cells. On the other hand, IL-10 is a potent cofactor for proliferation of human B cells and affects the B cell differentiation and isotype switching (1).
The role of IL-10 in glomerulonephritides (GNs) has been investigated in several studies with conflicting results. The administration of IL-10 (2), endogenous IL-10 (3), or IL-10 gene transfer (4, 5) diminished Th1 response and attenuated glomerular injury in murine crescentic GN initiated by a planted antigen. IL-10 administration also inhibited passive anti-glomerular basement membrane (GBM) GN (6) and suppressed mesangial cell proliferation in anti-Thy 1 GN in rats (7). More recently, adenovirus mediated IL-10 transfer had effects on prevention of the development of glomerulosclerosis in FGS/Kist mice model (8). Yin et al. (9) reported IL-10 gene deficiency evoked more severe lupus nephritis and higher mortality in murine lupus model. But in other experiments, IL-10 administration induced mesangial cell proliferation with transient reduction of creatinine clearance (10) and had no protective effects on passive anti-GBM GN in rats (11). Moreover, IL-10 up-regulated MHC class II expression by rat mesangial cells (12) and anti-IL-10 antibodies administration diminished the severity of GN in "lupus-prone" mice (13). In human GN, increase in tubulointerstitial expression of IL-10 was accompanied by nephrotic-range proteinuria (14). We also observed that the increased intrarenal expression of IL-10 was associated with tubular atrophy and interstitial fibrosis in renal biopsies from patients with IgA nephropathy (15).
The gene encoding IL-10 has been mapped to chromosome 1q and several polymorphic sites within the promoter region have recently been described (16). Three biallelic polymorphisms within the IL-10 promoter region, at positions -1,082, -819, and -592 from the transcription initiation site, have also been identified and one of these polymorphisms, at position -1,082 from the transcription initiation site, was shown to affect the in vitro IL-10 protein production in peripheral blood cells from healthy individuals (17).
Based on the aforementioned biological effects of IL-10 and its role in GN, inter-individual differences in the levels of IL-10 production resulting from promoter polymorphism could influence the individual predisposition to several autoimmune diseases, including glomerulonephritides. Increased frequency of the GA/AA genotypes at position -1,082 of the IL-10 promoter was reported in patients with several autoimmune diseases (18, 19). In fact, IL-10 promoter polymorphism was associated with renal involvement in southern Chinese patients with systemic lupus erythematosus (20). Low IL-10 producer genotype was more prevalent in Caucasian kidney transplant recipients than in the control population (21). We also observed a lower frequency of G allele at position -1,082, denoting high IL-10 producer, in Korean kidney transplant recipients compared with the healthy controls (22). Glomerulonephritis is the most common cause of renal failure in Korean kidney transplant recipients (23). In addition IgA nephropathy and focal segmental glomerulosclerosis is two most common glomerulonephritis leading to end stage renal failure in Korea. It is therefore possible that IL-10 promoter polymorphisms may be responsible for, at least in part, a portion of the genetic predisposition to glomerulonephritides. The present study was undertaken to investigate the role of these 3 biallelic IL-10 promoter polymorphisms in Korean patients with IgA nephropathy (IgAN) and focal segmental glomerulosclerosis (FSGS) which were common GNs leading to the end stage renal disease and considered to have different pathogenetic mechanism apart from each other.
MATERIALS AND METHODS
Patients and control subject
Patients were recruited from the Department of Internal Medicine, Kangdong Sacred Heart Hospital, and Seoul National University Hospital in Seoul, Korea. One hundred and eight patients with primary IgAN and forty nine patients with primary FSGS who provided informed consent, were enrolled in this study. The diagnosis of IgAN and FSGS was based on the typical light, immunofluorescent, and electron microscopic changes on a renal biopsy. Patients with the evidences of systemic diseases such as diabetes, chronic liver disease, and systemic lupus erythematosus were excluded. One hundred randomly selected subjects who had no evidence of renal disease and were normotensive were also recruited from the Health Promotion Center of the same hospitals as controls. The Institutional Review Board of two institutions approved the research protocol used for this study.
Extraction of genomic DNA and genotype determination
Genomic DNA was extracted from the buffy coat using commercial DNA isolation kit (Qiagen, Germany). The 3 biallelic IL-10 promoter polymorphisms were detected by PCR amplification followed by restriction enzyme digestion basically as described previously (24). Briefly, the DNA fragment containing the position -592 was amplified in 50 µL reaction mixture containing 500 ng of template DNA, 0.5 µM of of each primer, 1.5 mM of MgCl2, 200 µM each of dGTP, dATP, dTTP and dCTP, 2.5 unit of Taq polymerase (Promega, Medison WI, U.S.A.) and Taq polymerase buffer. Amplification of the fragment around -592 was performed under the same condition except that a final concentration of 2 mM MgCl2 was used. Amplification of fragment around -1,082 was performed using HotStarTaq kit (Qiagen, Germany), and Q-solution was included in the PCR reaction mixture. Primers used were as follows: for the amplification of -592 fragment, sense primer 5'gtgttcctaggtcacagtga, antisense primer 5'gtcatggtgagcactacctga 3'; for -819, sense primer 5'tcattctatgtgctggagatg 3', antisense primer 5'tgggggaagtgggtaagagt 3'; for -1,082, sense primer 5'ctcgctgcaacccaactggc 3', antisense primer 5'tcttacgcaacccaactggc 3'. PCR was performed using Perkin Elmer Cetus thermocycler under the following cycling parameters: denaturation at 94℃ for 2 min, followed by 35 cycles of denaturation at 94℃ for 30 sec; annealing at 60℃ for 45 sec; and extension at 72℃ for 1 min. This was followed by final extension at 72℃ for 10 min. For amplification of the -1,082, an initial activation step of 95℃ for 15 min preceded the cycling program. The two alleles at each polymorphic site was identified by incubating 15 µL aliquot of the PCR product with specific restriction enzyme, followed by electrophoresis on 3% agarose gels. Restriction enzyme RsaI cut the fragment at the position -592 when allele A was present, giving rise to 176 and 236 bp fragments. In the presence of allele C in -819 fragment, 125 and 84 bp fragments were generated by digestion with MaeIII. Mnl I cut -1082 fragment when allele G was present to generate 106 and 33 bp fragments. The results of this restriction fragment length polymorphism assay were confirmed by direct sequencing of the promoter region of the IL-10 gene in 10% of patients and controls (Macrogen Inc., Seoul, Korea).
Statistical analysis
All data were analyzed using the SPSS version 10.0. The chi-square test was used for detecting differences in the genotype distribution of the patients and controls. Odd ratio for individuals with a specific genotype to develop GN was estimated by Mantel-Haenszel test. A p-value that was less than 0.05 was considered to be statistically significant.
RESULTS
Allele frequencies of IL-10 promoter
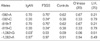
Frequencies of the alleles of IL-10 promoter in our patients and controls were summarized in Table 1. For comparison, reported allele frequencies from southern Chinese (20) and U.K. white population (25) were also included. The polymorphisms at -592 and -819 bp were found to be in complete linkage disequilibrium. This meant that individuals with A allele at -592 bp also had T allele at -819 bp, whereas those with C allele at -592 bp also had C allele at -819 bp. The allele frequencies of our controls were very similar to those of Chinese population but markedly different from U.K. population. To point out, the frequency of G allele at position -1,082 was markedly lower among our controls than the U.K. population.
For IgAN patients, the frequency of G allele at position -1,082 was even significantly lower than the control (p=0.006). For FSGS, the frequency of C allele at position -592 or at position -819 was significantly lower than the control (p=0.026).
Haplotype frequencies of IL-10 promoter
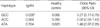
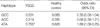
Three haplotypes were identified: GCC, ACC and ATA for the -1,082, -819 and -592 polymorphisms, respectively. The frequencies of the haplotypes of IL-10 promoter in IgAN, FSGS patients and controls were summarized in Table 2, 3.
There was a statistically significant difference in the frequency of GCC haplotype between IgAN and control. That is, IgAN patients were less likely to carry GCC haplotype than normal controls (0.028 vs. 0.095, p=0.006). FSGS patients were less likely to carry GCC haplotype than controls, although this did not reach a statistical significance (0.031 vs. 0.095). Besides, FSGS patients had a higher frequency of ATA haplotype than normal control (0.755 vs. 0.620, p=0.026).
Genotype frequencies of IL-10 promoter
From our subjects, we observed five genotypic combinations of the three haplotypes: GCC/ACC, GCC/ATA, ACC/ACC, ACC/ATA and ATA/ATA. No GCC homozygous subjects were observed from our study (Table 4).
No patients among the IgAN and FSGS group carried GCC/ACC genotype, while 8 (8%) among normal control group carried this genotype. This marked a statistical difference either between IgAN and control (p=0.002) or between FSGS and control group (p=0.049). There was no significant difference in the frequency of GCC/ATA genotype either between IgAN and control group or between FSGS and control group. However, as for the genotypic frequency of intermediate producer as a whole (i.e., GCC/ACC and GCC/ATA genotypes), there was a significant difference either between IgAN and control (p=0.005) or between FSGS and control group (p=0.048).
DISCUSSION
Three biallelic polymorphisms at positions -1,082(G/A), -819 (A/T) and -592 (A/C) of IL-10 promoter region are generally known to produce three haplotypes: GCC, ATA and ACC. Such allelic or haplotypic difference correlated with the difference in in vitro IL-10 production after various immunological stimuli. Even though not confirmed in recent study (26), Turner et al. reported that the presence of -1,082*A allele was associated with lower production of IL-10 by mitogen-stimulated peripheral blood leukocyte (17). In addition, the -592*A allele was associated with a reduced IL-10 production by peripheral blood mononuclear cell in the presence of IFN-γ (27). Some authors classify IL-10 haplotypic variations into high, intermediate and low producers (28, 29). GCC homozygous patients were considered as high producers (i.e., GCC/GCC genotype), GCC heterozygous patients as intermediate producers (i.e., GCC/ACC and GCC/ATA genotypes) and GCC negative patients as low producers (i.e., ATA/ATA, ACC/ATA and ACC/ACC genotypes)
In this study, we analyzed the polymorphic frequencies of the IL-10 promoter regions in Korean patients with IgAN and FSGS. We found that the distribution of alleles of IL-10 promoter in Korean healthy population is very similar to those in southern China population, but markedly different from Caucasian, which is consistent with the previous reports (17, 20, 24, 25). Characteristically, none of our controls and patients have the -1082*GG genotype or GCC/GCC genotype. This might mean that there was no one with "high IL-10 producing" phenotype among our subjects-either among the GN patients or among the healthy control.
The frequencies of -1,082*G alleles, which were reported to be related with a higher IL-10 production (17, 28, 27), were lower in patients with IgAN than healthy controls. The frequencies of -819*C and -592*C, which are also known to represent a high producer, were also lower among FSGS than the control (Table 1).
With respect to the haplotypes (Table 2, 3), there was a lower frequency of GCC haplotype among IgAN patients than the control (p=0.006, OR=0.27, CI [0.11-0.70]). FSGS patients were also less likely to carry the GCC haplotype, although not reached a statistical significance. ATA haplotype, which is known to represent a low producer, was more frequent among FSGS than control (p=0.026, OR=1.89, CI [1.09-3.25]).
Such genetic difference is more pronounced in terms of the genotype (Table 4). None of our IgAN or FSGS group carried the GCC/ACC genotype, which marked a stark difference in comparison with the control group with 8% frequency of the GCC/ACC genotype. Such statistical difference still holds in terms of the intermediate producer group, GCC/ACC and GCC/ATA genotypes, as a whole. Collectively, these findings might mean that the lower level of IL-10 production resulting from IL-10 promoter polymorphism predisposes individuals to the development of IgAN and FSGS.
Our findings are very similar to the study of Mok et al. (20) who demonstrated lower frequencies of -579*CC/-824*CC genotype and non-ATA haplotype in SLE patients with renal involvement. It was very interesting to note that IL-10 promoter polymorphisms predispose individuals to 3 different GNs, IgAN, FSGS, and lupus nephritis, which have an independent immunological pathogenesis. In addition, the frequency of -1,082*AA genotype was more prevalent in Caucacian kidney transplant recipient than in control group (21). In our 185 kidney transplant recipients, the frequencies of -592*CC/-819*CC and -1082*GA genotype were 9.2% and 5.9% respectively, which were lower than in controls (22). In this regard, it might be worthwhile to investigate the role of IL-10 promoter polymorphism in other nephropathies such as membranous GN, membranoproliferative GN and even diabetic nephropathy which are common causes of end stage renal disease.
The biological effects of IL-10 and the role of IL-10 in GN is very complex and is beyond the scope of our discussion. From the results of the present study, it may be speculative that IL-10 limits inflammation and modulates injuries to kidney initiated by various different mechanisms. In this respect, IL-10 may play an important role in the process of progression common to both IgA nephropathy and FSGS. Recently IL-10 high producer genotype was reported to be associated with slower progression of IgA nephropathy and FSGS in Caucasian patients (30). Because our study was a cross-sectional study with a great variability in follow-up duration and patient characteristics affecting the progression of glomerulonephritis, we could not analysis the association of IL-10 gene polymorphism and progression of diseases. Well-designed prospective long-term study will be necessary to evaluate the role of IL-10 in the progression of various primary and secondary glomerular diseases having different mechanisms of pathogenesis such as IgA nephroapthy, FSGS, membranous nephropathy, lupus nephritis, and diabetic nephropathy.
Finally, a cytokine works in the context of "networks of cytokines" i.e. many cytokines influence each other. The role of gene polymorphisms of various cytokines other than IL-10 in GN has been reported (31-33) and allelic distributions in cytokine gene polymorphisms varied according to the ethnic groups (25). In this context, it might be necessary to examine our observation as to the effect of IL-10 promoter gene polymorphism on the development of GN in different ethnic populations.

 XML Download
XML Download