

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The intrapulmonary bronchogenic cyst appears a sharply circumscribed, round or oval nodule or mass, usually in the medial third of the lungs. The lesion do not communicate with the tracheobronchial tree until they become infected, a complication that occurs in about 75% of cases recognized clinically (1, 2). Bronchial polyps are rare findings and classified as multiple papillomas, solitary papillomas, and inflammatory polyps (3). Bronchial polyp occurs spontaneously or after airway injury such as chronic infection, foreign bodies, asthma, and inhalation injury. We report a case of polypoid intrapulmonary lung cyst, which was the first case among Koreans, has been removed by bronchoscopy.
CASE REPORT
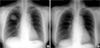
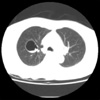
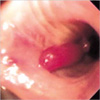
A 68-yr-old woman came to our hospital with a month history of discomfort and pain in the right upper chest. She denied a history of fever, upper respiratory infection, or allergies. She had never smoked. On admission her blood pressure was 120/80 mmHg, pulse rate 84/min, respiratory rate 24/min, and body temperature 36.6℃. Cardiac examination showed normal findings. The lungs on auscultation showed a decrease in vesicular sounds in the right upper lung field. Laboratory tests revealed normal findings. On spirometry, her forced vital capacity and forced expiratory volume in 1 sec were 2,480 mL (120% of the predicted value) and 2,000 mL (139% of the predicted value), respectively. Chest radiography revealed cystic lesion in the right upper lung (Fig. 1A). Computed tomography revealed a 4×5 cm sized large cyst before polypectomy (Fig. 2). Neither enlarged mediastinal lymph nodes nor extrabronchial involvements were observed. Flexible bronchoscopy revealed a peduncular polyp about 2 cm in length originating from the anterior segment of the right upper lung (Fig. 3). The surface of the polyp was smooth. After bronchoscopic removal with biopsy forceps of the polyp, cystic lesion of the right upper lung disappeared (Fig. 1B) and the discomfort and pain in the right upper chest of patient improved. Gross appearance showed polyp with stalk and light-microscopical examination showed a lymphocyte infiltration with epithelial lining cells that was consistent with the diagnosis of a bronchial inflammatory polyp (Fig. 4).
DISCUSSION
This is a rare case of polypoid intrapulmonary bronchogenic cyst, which was disappeared after bronchoscopic removal. There were possible diagnoses for the initial radiographic chest findings of the cystic lesion in the right upper lung, including infected cyst, infected large bullae, pulmonary sequestration. After bronchoscopic removal, the right upper cystic lesion disappeared immediately. Bronchogenic cysts are usually solitary, thin walled, unilocular, and roughly spherical in shape. They are filled with either mucoid or serous fluid and do not communicate with the tracheobronchial tree unless they become infected, in which case the cyst fluid may be pus or by pus and air (4). In this case cystic fluid is not aspirated during bronchoscopy. The cyst wall often contains cartilage and respiratory epithelium. Most are discovered incidentally and cause no symptoms. However they may communicate with the tracheobronchial tree and become infected and some enlarge to cause airway obstruction. Bronchial polyps are classified as multiple papillomas, solitary papillomas, and inflammatory polyps (3). Inflammatory polyps of the airways are now regarded as histopathologically distinct nonneoplastic endobronchial lesions, which in adults are associated with a variety of chronic inflammatory insults such as chronic infection, foreign bodies, asthma, or inhalation injury (5-7). Generally, benign bronchogenic cysts need not be resected unless they cause symptoms. In treatment of bronchial polyp there are several methods such as bronchoscopic excision and lobectomy. The developments in bronchoscopic techniques have made it possible to remove superficial tumors by bronchoscopy. Removal of the foreign body or inhalation of corticosteroid may resolve bronchial polyp (5). In the present case, bronchial polyp was removed by bronchoscopy and then lung cyst disappeared suggesting that intrapulmonary cyst communicate with bronchus. Histologically the bronchogenic cyst wall is lined by a pseudostratified, ciliated epithelium and contains cartilage and strands of smooth muscle important for diagnosis. In the present case, polyp composed of epithelial lining cells without cartilage in their wall may represent intrapulmonary cyst as a result of ingrowth from communicating airway epithelium.

 XML Download
XML Download