INTRODUCTION
According to the annual Report of the Korean Central Cancer Registry (1), the total number of cancer patients registered in Korea is approximately 90,000 (2). Pain is the most common and offensive symptom in cancer patients, and pain without the hope of relief severely damages their quality of life.
A multi-center study with general or university hospitals showed that 52.1% of cancer patients suffer from pain, and 62.6% among them are not satisfied with the current pain control (2). This might be attributed to the patients themselves, the social system, and cultural perspectives but some responsibility can be leveled at the medical care team that does not evaluate the cancer pain properly. Pain is regarded to be the 5th vital sign, and establishing a treatment plan according to the pain intensity is essential (2).
Pain is an unpleasant experience related to the substantial or potential tissue damage (3). Cancer pain was explained by the concept of "total pain" (somato-pshychic experience) by Saunders (4) and can be affected by physical factors as well as psychosocial and spiritual factors. Therefore, understanding the mental, social, spiritual and physical problem is fundamental, and it is the most important first step in cancer pain management. Because pain is a subjective symptom, an appropriate and objective cancer pain assessment tool, with a proven reliability and validity, is needed and the descriptions of pain by the patients need to be trusted.
The initial assessment of cancer patients must be focused on elucidating the cause of the pain and establishing a management plan. For this purpose, the control of cancer pain should be done with a continuous assessment of the pain with consideration of the psychosocial aspects as well as the quality, initiation, changes over time, history of management, and desire to control the pain.
There are several pain assessment tools such as the Visual Analogue Scale (5), the Verbal Numeric Rating Scale (5), the Verbal Rating Scale (6), the Faces Pain Scale (7), the Brief Pain Inventory (8), the Memorial Pain Assessment Card (9) and The McGill Pain Questionnaire (10). However, these assessment tools cannot be applied to Koreans with any hope of meaningful analysis because, besides the issues of copyright, reliability and validity, they were merely translated after being developed in a completely different cultural background. Therefore, the 'practical committee for cancer pain assessment tool' was organized in August 2002. By May 2003 'Korean Cancer Pain Assessment Tool' (KCPAT) was developed after 20 meetings at consultant conferences (11). The KCPAT consists of the following 1) the location of the pain using a body chart, 2) the nature of the pain and the pain intensity using the pain expression descriptions, 3) the current pain intensity using the Visual Analogue Scale (VAS), 4) the accompanying symptoms affecting the pain, and 5) psychosocial items affecting the pain.
The validity and reliability of the 'KCPAT' was assessed.
MATERIALS AND METHODS
Subjects
According to the 2001 Korean Cancer Central Registry Report, there were Korean 91,944 cancer patients (2001). There were 51,753 (56.3%) males and 40,191 (43.7%) females. 90,252 patients were chosen for the population of this study after excluding those patients with an unknown address, age <18 yr (1,673 persons) and those who were not contactable. Among the study population, 903 patients (1%) were selected as the study sample. An investigation of whole study subjects was performed in a tertiary hospital (mainly university hospitals) from May to August 2003.
Sampling method
A stratified proportional-quota and clustered systematic sampling method were used to sample the study population. After stratifying the entire country to various administrative sectors, a sample number proportional to the target population was allocated to a stratified area. An oncologist was selected from each university hospital in each group, which was considered to be a cluster. The oncologists selected were requested to interview the cancer patients, regardless of gender, age, and type or stage of cancer using the systemic sampling method as follows (Table 1).
The systemic sampling method given to the oncologists was as follows:
"Please, divide the one week's number of patients including the hospitalized and out-patients (regardless of gender, age, and type or stage of cancer) by the number of interviewees allocated to you.
For example, if the total number of patients seen by you in a week is 50 and the number of interviewees allocated to you was 12, the selected number would be 4 (50/12=4.17 → In the case of 4.17, 4 is chosen). Then, apportion a temporary serial number to each patient. After choosing a number from 1-4, interview the patient whose number is the sum of 4 and the chosen number. For example, if number 1 is chosen, the patients numbered 1, 5, 9, 13, 17, 21, 25, 29, 33, 37, 41, and 45 should be interviewed. If number 3 is chosen, patients whose numbers are 3, 7, 11, 15, 19, 23, 27, 31, 35, 39, 43, and 47 should be interviewed etc. This method established the representation of the sample regardless of gender, age and the type or stage of cancer. In the case of patients age below 18 yr, no current pain at interview, and where communication was difficult, the next patient in the series should be interviewed."
RESULTS
Demographic characteristic of subjects
The response rate was 34.8% with 314 people from 903 subjects. 170 persons (54.1%) were male and 144 (45.9%) were female (the male to female ratio of the total cancer patients was 1.29). The mean age was 56.34±11.78 yr, 57.0±11.3 yr in males, and 55.6±12.4 yr in females. The majority of patients had a metastasis (217 persons, 71.6%) and was hospitalized (255 persons, 81.5%).
Reliability of KCPAT
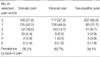
The reliability of the questionnaire could not be measured by Cronbach-alpha because the items were not structured separately. However, the inner consistency was checked by the correlation of the 'average pain score along the pain nature (somatic pain, visceral pain, neuropathic pain) on a 5-point on Likert scale' and the 'present pain intensity on the VAS'.
The mean pain score was 3.01±1.10 in the patients complaining of pain. The mean score was 3.13±1.00 (214 persons) in those with somatic pain, 2.96±1.11 (197 persons) in those with visceral pain, and 2.83±1.03 (106 persons) in those with neuropathic pain.
The present pain intensity evaluated on the VAS was 4.51±2.49 and it showed an internal consistency (r=0.560, p<0.0001). When the pain score along with the nature of the pain was compared with the pain score on the VAS, the agreement of the mean score was 0.364±0.0344 in Kappa (95% CI=0.302-0.437) (Table 2).
Validity of KCPAT
The oncologist, family doctor, pain vocabulary specialist, hospice nurse, social worker, Korean language scholar, English language scholar, medical statistician and a social psychologist provided the specialist validity. The questionnaire was developed after many conferences examining several foreign questionnaires with proven reliability and validity.
The investigators were requested to write down any expression of pain besides the 5 pain descriptions used in previous research. The descriptions, reported by more than 10% of the respondents, were examined for the content validity under a 90% confidence level. In the case of psychosocial and accompanying symptoms, the content validity was examined by checking for any items beyond 10% in the other opinions besides the selected items. The practical committee also reordered the questions according to frequency of pain expression. A particular pain expression with a frequency exceeding 20% was added to each section.
The frequency of the 5 selected expressions of somatic pain was as follows: 'throbbing' (109 persons, 36.0%), 'tight' (79 persons, 26.1%), 'splitting' (50 persons, 16.5%), 'tearing' (37 persons, 12.2%), and 'stabbing' (28 persons, 9.2%).
The prevalence of somatic pain was 68.2% (214 persons/314 persons). The number of pain descriptions selected was 1 in 135 patients (43.0%), 2 in 53 patients (16.6%), 3 in 20 patients (6.4%), 4 in 2 patients (0.6%), and 5 in 5 patients (1.6%) (Table 3). The number of other descriptions about the somatic pain was 15. The frequency of the other descriptions is as follows: 'heavy' (6 persons, 40%), 'dull' (3 persons, 20%), 'crushing' (2 persons, 13.3%), 'tightness' (1 person), 'ache' (1 person), 'exploding' (1 person), and 'taut' (1 person). 'Heaviness', which was the most frequent answer, was added to the questionnaire.
The frequency of the 5 selected expressions of visceral pain is as follows: 'ache' (88 patients, 34.8%), 'throbbing' (52 patients, 20.6%), 'sore' (42 patients, 16.6%), 'wrenching' (38 patients, 15.0%), and 'cramping' (33 patients, 13.0%). The prevalence of visceral pain was 62.7% (197/314 persons). The number of selected pain descriptions was 1 in 138 persons (44.0%), 2 in 43 persons (13.7%), 3 in 9 persons (2.9%), 4 in 1 person (0.3%), and 5 in 6 persons (1.9%) (Table 3). The number of other visceral pain descriptions was 21. The frequency of the other descriptions is as follows: 'heavy' (5 persons, 20%), 'dull' (3 persons), 'tightness' (3 persons), 'pulling' (3 persons), 'stinging' (2 persons), 'pricking' (1 person), 'breaking' (1 person), 'cutting' (1 person), 'smarting' (1 person), and 'pounding' (1 person). 'Heaviness', which was the most frequent answer, was added to the questionnaire.
The frequency of the 5 selected descriptions of neuropahic pain is as follows: 'numbness' (50 persons, 30.1%), 'tingling' (39 persons, 23.5%), 'burning sensation' (32 persons, 19.3%), 'shooting' (24 persons, 14.4%), and 'allodynia' (21 persons, 12.7%). The prevalence of neuropathic pain was 34.1% (107/314 persons). The number of pain descriptions selected was 1 in 68 persons (21.7%), 2 in 21 persons (6.7%), 3 in 9 persons (2.9%), 4 in 3 persons (0.9%), and 5 in 6 persons (1.9%) (Table 3). Additional descriptions were not chosen because there was no answer occurring more frequently than 20%.
The frequency of the 10 items of accompanying symptoms besides pain using the 'Memorial Symptom Assessment Scale' is as follows. 'anorexia' (194 persons, 17.6%), 'inertia' (177 persons, 16.0%), 'sleep disturbance' (128 persons, 11.6%), 'thirsty' (106 persons, 9.6%), 'weight loss' (106 persons, 9.6%), 'constipation' (10 persons, 9.2%), 'decreased concentration' (95 persons, 8.6%), 'dizziness'(92 persons, 8.3%), 'sleepy' (71 persons, 6.4%), and 'itching sensation' (34 persons, 3.1%). The number of other descriptions was 25, which were as follows: 'nausea' (5 persons, 25%), 'cough' (3 persons, 12%), breathing difficulty (2 persons), diarrhea (2 persons), dyspnea (2 persons), difficulty in micturation (2 persons). 'Nausea' and 'cough' were added to the questionnaire because their frequency was >10%. 'Thirsty' was changed to 'dry mouth'.
The frequency of the 8 psychosocial items is as follows: 'support from family' (171 persons, 26.1%), 'compliance for pain killer' (245 persons, 23.7%), 'response type to stress' (156 persons, 15.1%), 'current emotional state such as anxiety or depression' (142 persons, 13.7%), 'spiritual suffering on current state of patient oneself' (91 persons, 8.8%), 'ability or inability of self control' (86 persons, 8.3%), 'drug dependency or addiction' (38 persons, 3.7%), and 'past history of psychiatric illness' (6 persons, 0.6%). The order of the psychosocial items was adjusted according to the answer frequency.
Satisfaction on KCPAT
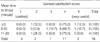
Twenty-six oncologists participated in the inquiry, 12 (46.2%) from Seoul, 3 (11.5%) from Kyungi province, 2 (7.7%) from Gangwon province, and one person each from Busan, Daegu, Incheon, Gwangju, Daejeon, Ulsan, Chungnam, Jeonbuk, and Gyeungbuk. Twenty of the oncologists (76.9%) were male and 6 (23.1%) were female. The mean age of the respondents was 39.8±6.34 yr. The average completion time of the questionnaire was 8.9±5.29 min in 18 respondents and the satisfaction level was 3.8±0.79 (5-point Likert scale). The correlation of the average completion time and the satisfaction level is shown in Table 4.
DISCUSSION
KCPAT can be used for initial cancer pain assessment by interviewer. It consists of the following: 1) the location of the pain using a body chart, 2) the type of the pain and the pain intensity using the pain expression descriptions, 3) the present pain intensity using the Visual Analogue Scale, 4) the accompanying symptoms affecting the pain, and 5) psychosocial items affecting the pain. The patents can respond with the plural form on each item with the exception of item 3. The KCPAT also can be used in a periodic reevaluation after medical intervention. The intensity of the pain can be checked with the 'average pain score along the pain nature' and 'present pain score'.
The descriptions used in the KCPAT were corrected based on the reliability and validity examined, and they were also reordered according to the frequency of the answers. After modifying the questions, an evaluator's manual was produced. The completion time of the KCPAT was less than ten minutes.
Although pain is common problem in cancer patients, the management of pain is still inappropriate in Korea (12). This inappropriate management of pain is mainly due to the lack of pain assessment tool as well as lack of education for assessing the pain (13-15).
The KCPAT was developed to evaluate the cancer pain in Korean adults and it is a tool consistent with the total pain concept. Lee et al. reported that the average pain score was 3.80 (0-10 point scale) and the satisfaction score on cancer pain management was 4.19 (1-6 point scale) (11).
The background of developing KCPAT is increasing national interest of cancer pain. The interest of cancer pain make it possible to develop the guideline for cancer management by the Korean Society of Hospice and Palliative Care (2).
Oncologists who evaluated cancer pain using the KCPAT reported the possibility of an overestimation in the case of incidental pain, the need for diversifying the pain descriptions, supplementing the content for the continuous evaluation of pain, and analyzing the level of pain control by observing the response after the pain control measure.
There were some limitations in this study. The first is that discriminating the pain nature was difficult due to the difference in knowledge and expression between doctors and patients. The second is the difficulty in delivering a psychological concept even with the provision of an evaluator's manual. The third is that pain can be under or overestimated because the pain duration was not written in the questionnaire, the 'Average pain score along with the nature' might reflect only the current pain intensity.
Although there are some limitations, the importance of this study is that KCPAT is the first qualitative and quantitative pain assessment tool that was developed in Korean language. Therefore, the effect of KCPAT is extensive in the part of education for physician without mentioning the assessment of cancer pain. In addition, even though the KCPAT was developed for evaluating cancer pain, it can also be used as a basis for future treatments by reducing the administration of unnecessary medications and operations. Moreover, it will contribute to an evaluation of the quality of life of cancer patients because it can assess the efficacy of the treatments. However, a simpler tool that is more appropriate for a clinical setting and one that patients can complete by themselves needs to be developed. With this continuous feedback, the KCPAT can be revised and improved.