

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cardiovascular disease is the leading cause of mortality among patients with end-stage renal disease. A carotid intima-media thickness of >0.9 mm and the presence of discrete plaques are each considered markers of generalized atherosclerosis, and are associated with cardiovascular risk factors (1, 2).
Vascular calcifications are common in patients with end-stage renal disease (3). Such calcifications are believed to arise from calcifications of the intimal layer of the vessel caused by atherosclerotic changes, or calcifications of the medial wall that correspond to Mönckeberg's arteriosclerosis (4). There is strong evidence that calcifications contribute to cardiovascular mortality not only in renal patients but also in patients with non-insulin-dependent diabetes mellitus (DM), as well as in the general population (5, 6).
One study reported that in end-stage renal disease, increased intima-media thickness and presence of calcified plaque occurs not only in central elastic arteries such as the aorta and carotid but also in peripheral muscular-type arteries including the femoral (7). Furthermore, carotid artery intima-media thickness is linked to left ventricular hypertrophy in dialysis patients (7). These findings suggest that some cardiac and vascular changes may occur in parallel in dialysis patients.
There are two reports (8, 9) on the prevalence and significance of a thickened intima-media layer and the presence of arterial plaques in patients undergoing continuous ambulatory peritoneal dialysis (CAPD) in Korea. The present study examined intima-media thickness and carotid and brachial artery plaque prevalence in CAPD patients and healthy normotensive controls. The study also sought to determine whether cardiac and vascular changes occurred in parallel in dialysis patients. We therefore investigated the prevalence of vascular calcifications and survival rates during 2-yr follow-up in 25 CAPD patients in a single dialysis center.
MATERIALS AND METHODS
Patients
The study involved 50 subjects in total. Group 1 consisted of 25 CAPD patients (14 men, 11 women; mean age 59±11 yr) without clinical vascular disorders in a mean time undergoing CAPD of 35 months (4-120 months). Group 2 consisted of 25 age- and sex-matched controls. Exclusion criteria were patients with histories or signs of cardiac failure, unstable angina pectoris, peripheral vascular disease, systolic blood pressure >180 mmHg or diastolic blood pressure >105 mmHg, serum albumin <2.5 g/dL, intact-PTH level >200 pg/mL, serum total calcium level >11 mg/dL or serum phosphate level >7 mg/dL. Primary kidney disease patients comprised 14 with diabetes mellitus (DM) and 11 non-DM patients (Table 1).
Methods
Three distal wall measurements were taken to determine the intima-media thickness of the common carotid artery and brachial artery. These measurements were taken within 1 cm of the bifurcation using a high resolution B-mode duplex ultrasound imager (7.5 MHz transducer, Hewlett-Packard, Sonos2000®, Bothell, Washington, U.S.A.) by the same trained cardiologist on each occasion, and the mean of these measurements was used in analysis. Intima-media thickness was defined as the distance from the leading edge of the lumen-intima interface of the far wall to the leading edge of the media-adventitia interface of the far wall, as validated by Pignoli et al. (10).
The intima-media cross-sectional areas (IMCSA) of the common carotid and brachial arteries were calculated as follows:
-
-IMCSA=[π(D/2+IMT)2-π(D/2)2]
(D=artery diameter at end-diastole, IMT=intima-media thickness) (11)
Atherosclerotic plaques were classified as fibrous, mixed or calcified based on comparisons made between B-mode ultrasound observations of plaques (12, 13). Bright white echoes denoted plaques of greater density, and represent mineralization and calcification. Patients were allowed to take regular medication. The same nurses consecutively (5 times) measured sitting blood pressure conventionally with a sphygmomanometer on the left side. The systolic blood pressure and diastolic blood pressure data shown in the study represent the means of these 5 measurements. Mean arterial pressure was calculated using the following formula, 'systolic blood pressure+2×diastolic blood pressure)/3', while pulse pressure was calculated in the following manner, 'systolic blood pressure-diastolic blood pressure'.
Baseline echocardiography was performed using a Hewlett-Packard Sonos 100 device equipped with a 2.25-MHz probe, allowing M-mode, 2-dimensional and pulsed Doppler measurements. Measurements were made according to the recommendations of the American Society of Echocardiography. Left ventricular mass was calculated according to the Penn convention equation (14). Left ventricular hypertrophy was defined as left ventricular mass index >125 g/m2 (7).
In the CAPD patient group, blood samples were analyzed for phosphorus and total calcium concentration using an Hitachi 747 automatic analyzer, with normal ranges considered as being 1.9-4.4 mg/dL and 8.2-10.4 mg/dL, respectively. Intact-PTH was measured using a commercial immunoradiometric assay (Diagnostic products corporation, Los Angeles, CA, U.S.A.), and the normal range in our laboratory is considered to be 12-72 pg/mL. Serum albumin was measured using an Hitachi 736-740 autoanalyzer (Hitachi Ltd, Tokyo, Japan), and C-reactive protein was measured using a COBAS INTEGRA (Roche Diagnostic Systems, Somerville, NJ, U.S.A.). Serum total cholesterol, LDL-cholesterol, HDL-cholesterol and triglyceride levels were measured by enzymatic methods using an Hitachi 736-740 autoanalyzer. Just before the examination echocardiography, all subjects had fasting blood samples for above examinations. For patients, additional analysis of the mean of the previous six samples over the preceding 6-month period was also included.
To evaluate the total Kt/V urea index (Kt/V) in CAPD patients, the sum of 24 hr residual and dialytic urea clearances was divided by the urea distribution volume which was calculated using Watson's nomogram. Residual renal function (RRF) was estimated using the average of the residual urea and creatinine clearances.
Parameters with Gaussian distribution are expressed as mean±SD; between-group differences were assessed for significance using unpaired t-tests and Mann-Whitney U tests as appropriate (SPSS Windows version 9.0). Parameters with skewed distribution are expressed as median and range; Wilcoxon and Kruskal-Wallis testing was used for comparing data from 2 groups. Dichotomized variables were compared using Pearson's chi-square test or Fisher's exact test. Spearman's correlation coefficients were used to express association between parameters. Differences were considered significant if the p value was less than 0.05.
RESULTS
Intima-media thickness, left ventricular mass index and calcified plaque occurrence in the common carotid and brachial arteries of CAPD patients and normal controls
We found that both the carotid and brachial artery intimamedia layers were thicker in the CAPD group compared to control group (carotid: 0.75±0.30 vs. 0.60±0.16 mm, p=0.003; brachial: 0.46±0.07 vs. 0.38±0.08 mm, p=0.002). Similarly, the mean carotid and brachial intima-media cross-sectional areas were greater in the CAPD group compared to control group (carotid: 64.4±31.5 vs. 44.5±11.6, p=0.03; brachial: 21.1±0.1 vs. 15.9±0.1, p=0.02). Compared to controls, the mean left ventricular mass index was higher in the CAPD group (168.0±60.8 vs. 99.0±20.7, p=0.04). The proportion of subjects with calcified plaques was also higher in the CAPD patient group compared to controls (14/25 (56%) vs. 2/25 (8%), p=0.01) (Table 2). We found that while 14 patients had discrete carotid artery calcified plaques, only three of these (2 males, 1 female) had a carotid intima-media thickness >0.9 mm.
Correlations between left ventricular mass index and intima-media thickness, and intima-media cross-sectional area in common carotid and brachial arteries
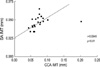
In CAPD patients, common carotid artery intima-media thickness correlated well with brachial artery intima-media thickness (r=0.5949, p<0.01) (Fig. 1). In CAPD patients, neither common carotid artery intima-media thickness nor common carotid artery intima-media cross-sectional area correlated with left ventricular mass index (r=0.167, p=0.54 and r=0.261, p=0.45, respectively), and similarly, neither brachial artery intima-media thickness nor brachial intima-media cross-sectional area correlated with left ventricular mass index (r=0.115, p=0.34 and r=0.056, p=0.78, respectively). In contrast, the left ventricular mass index was greater in CAPD patients with calcified plaques in the carotid artery (Table 3) and significantly correlated with carotid calcification (r=0.561, p=0.04).
Comparisons between CAPD patients with and without calcified plaques
Compared to CAPD patients without carotid artery calcified plaques, CAPD patients with such plaques had a greater incidence of diabetes mellitus (79 vs. 36%, p=0.04), greater C-reactive protein levels (16.5 (6.9-29.7) vs. 9.3 (3.0-16.1), p=0.02), higher left ventricular mass index (199±78 vs. 144±26, p=0.04) and a lower 2-yr survival rate (50 vs. 73%, p=0.04) (Table 3). All deaths in carotid calcified plaque patients comprised 4 cerebrovascular accidents, 2 ischemic coronary events and 1 death from peripheral vascular disease with sepsis.
DISCUSSION
The present study revealed an extremely high prevalence of advanced calcifying plaque in the carotid arteries of CAPD patients. Carotid calcifications were observed in 56% of CAPD patients compared to 8% of controls. These data are consistent with those of Savage et al. showing calcified plaques are common in the carotid arteries of CAPD patients without clinical vascular disease (7). Expectedly, we found that all of the calcified plaques were found in the carotid artery. In addition, we found that carotid and brachial artery intima-media thicknesses were greater than those of matched control subjects. Unexpectedly, intima-media thickness was not always associated with the presence of plaque in the same vessel.
Left ventricular hypertrophy has been shown to independently predict cardiovascular mortality in end-stage renal disease patients (15). Roman et al. reported a positive independent association between carotid intima-media thickness and left ventricular end-diastolic diameter (16). London et al. found both ventricular diameters and left ventricular mass correlated with carotid intima-media thickness (17). In the present study, common carotid artery intima-media thickness and intima-media cross-sectional area correlated well with those of the brachial artery. However, intima-media thickness and intima-media cross-sectional area of the common carotid or brachial artery did not correlate with left ventricular mass index. Indeed, the left ventricular mass index was higher in CAPD patients with calcified plaques in the carotid artery. Given these data refer to discrete calcified plaques rather than continuous plaques, it appears that calcification per se, especially in a central artery such as the common carotid, directly influences left ventricular mass index in CAPD patients. This hypothesis appears to be supported by the reports of both Guerin et al. and London et al. showing that the presence of vascular calcification was associated with increased stiffness in larger arteries, and that this stiffness may have important clinical consequences partly due to its association with increased systolic blood pressure and concentric left ventricular hypertrophy (11, 18). Moreover, increased stiffening of the large arteries was found to be an important predictor of mortality in renal patients (19). The present study found that the 2-yr survival rate in patients with carotid calcified plaques was lower than in patients without carotid calcified plaques. We found that all deaths in carotid calcified plaque patients were due to cardiovascular disease. According to Oh et al., end-stage renal disease patients have a high prevalence of vascular calcification associated with microinflammation, high PTH, calcium-phosphate product and homocysteine, but not traditional atherogenic risk factors (20). Hyperparathyroidism, calcium-phosphate overload and hyperhomocysteinemia are modifiable and treatable disorders. To elucidate the association between the above factors and vascular calcification, we conducted a study which excluded patients with uncontrolled hypertension, severe malnutrition, established infection, high serum intact-PTH and total calcium and phosphate levels. We found that CAPD patients with carotid artery calcified plaques had a greater incidence of diabetes mellitus and had higher C-reactive protein levels compared to CAPD patients without carotid artery calcified plaques. There were no positive correlations between carotid calcified plaques and other parameters such as age, sex, CAPD duration, intima-media thickness, hyperlipidemia, blood pressure and serum albumin level.
In addition to atherosclerotic changes, the vessels in DM patients are characterized by increased amounts of connective tissue such as fibronectin, collagen and glycoprotein, and increased amounts of calcium in the medial layer of the arterial wall. The pathogenesis and high prevalence of medial artery calcification in DM patients, also known as Mönckeberg's arteriosclerosis, remain the subjects of debate. Given the present study did not involve histological examination of the carotid or brachial arteries, we cannot state whether patients had reached the final stage of atherosclerosis, or whether a Mönckeberg's arteriosclerosis, as described previously in diabetic and uremic patients, was responsible for the prevalence of calcified plaques.
The acute-phase protein C-reactive protein is chronically elevated in one third to two thirds of dialysis patients (21). C-reactive protein is considered a surrogate marker of a microinflammatory state, and is a powerful predictor of general and cardiovascular mortality both in the general and in the end-stage renal disease population (21, 22). We demonstrated here that C-reactive protein levels were higher in carotid calcification patients. Multiple inflammatory mechanisms are implicated in the initiation and propagation of atherosclerotic lesions (23). C-reactive protein may be directly involved as it binds to degraded LDL particles, is deposited at the intima-media interface, co-localizes with complement, and attracts monocytes to atherosclerotic lesions (21). Moreover, calcification of vascular cells and atheromatous lesions is directly stimulated by TNF-α, a proinflammatory cytokine that also promotes C-reactive protein release (24). We believe that further study aimed at elucidating the mechanisms underlying the higher prevalence of vascular calcification in patients with DM and high C-reactive protein levels is warranted.
In conclusion, the present study revealed an extremely high prevalence of carotid calcification in CAPD patients without clinical vascular disorders. Patients with carotid calcification had a greater incidence of DM, higher C-reactive protein levels and left ventricular mass index, and a lower survival rate. Therefore, it appears that optimal peritoneal dialysis treatment should aim to reduce factors that contribute to inflammation, such as bioincompatibility of solutions, fluid overload, loss of residual renal function, increased body fat mass and peritonitis.



 XML Download
XML Download