

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acute allograft rejection is the most important factor for early graft loss and appears to increase the risk of graft failure in cadaveric kidney transplantation (1). Furthermore, non-immunologic factors such as donor and recipient's age, sex, donor source and immunosuppressive regimens influence allograft prognosis (2). Mycophenolate mofetil (MMF) is the morpholinoethly ester of mycophenolic acid (MPA).
MMF is rapidly converted into MPA after oral administration and absorbed in the gut. MPA is a potent, reversible, uncompetitive inhibitor of inosine monophosphate dehydrogenase, and thus MMF acts as a selective inhibitor of T- and B-cell proliferation by blocking the production of guanosine nucleotides and interfering with the glycosylation of adhesion molecules. Four clinical trials evaluated the efficacy of MMF in the prevention of renal allograft rejection, using the incidence of biopsy-proven acute rejection or treatment failure at 6 months after transplantation as the primary efficacy endpoint. Three of the four studies compared the triple-therapy regimen of cyclosporine (CsA), corticosteroids, and MMF (one study with and one study without anti-thymocyte globulin [ATG] induction) with a classic triple-therapy regimen composed of azathioprine (AZA) (with or without ATG), CsA, and corticosteroids (1, 3, 4). In the 4th study, MMF-based triple therapy was compared with a dual therapy consisting of placebo, CsA, and corticosteroids (5). All studies concluded that MMF reduced the incidence of biopsy-proven acute rejection or treatment failure significantly during the first 6 months.
Before the establishment of KONOS (Korean Network of Organ Sharing), February 2000, all the organ distributions of cadaver donors were the responsibility of the organ procurement hospital which is basically identical to transplantation hospital. Accordingly, only the following case was included in our study: when a cadaver turned up in our hospital and the recipient also underwent transplantation in our hospital. In order to evaluate how immunosuppressive agents such as MMF and AZA would influence the outcome of the graft kidney, we analyzed the incidence of acute rejection episodes, cytomegalovirus (CMV) infection within the first 6 months following renal transplantation and the 5 yr graft survival rate after minimizing the influences of donor factors by grafting from the same cadaveric donor.
MATERIALS AND METHODS
The study population consisted of 68 consecutively admitted patients who were grafted from 34 cadaveric donors from May 1998 to January 2000 at Samsung Medical Center. Pre-operatively, the study protocol was explained in detail to all patients and an informed consent to perform the study was obtained.
The experiment was carried out after factors involving donors, the operation itself and patient control following operation were minimized. When two cases of kidney transplantation took place from the same cadaveric donor in our hospital, transplantation was performed on a first come first served base. MMF was administered to the early-transplanted patient and AZA to the following patient, and vice versa in the next case. The patients orally received MMF (1.5 g/d) or AZA (100-130 mg/d) and the dose was regulated by the patient's conditions. If we suspect an acute rejection, graft biopsy was performed to diagnose the acute rejection. If it was not available, clinical impressions such as elevated serum creatinine level and decreased urine output, and radiological results supported by Doppler ultrasound were used for the diagnosis of acute rejection. Acute rejection, graft loss, death, and discontinuation of study drugs were defined as treatment failure. Patient and graft survival rates were compared between the two groups. In the case of graft nephrectomy or taking hemodialysis over 6 weeks post-transplant, they were categorized as graft loss. CMV antigenemia test and clinical evidence were used to compare CMV infection rate between the two groups. Patients who developed CMV disease or a high level of CMV infection (antigenemia assay >50/400,000 mononuclear cells) were treated with an antiviral agent such as gancilovir.
Kaplan-Meier method was used for the analysis of graft survival rate. Recipient's age, body weight, HLA mismatching, and cold ischemic time were tested by Mann-Whitney test between groups. Chi-square test was applied to evaluate sex and underlying disease variation. p-values less than 0.05 were considered statistically significant in all results.
RESULTS
In the comparison of demographics and clinical characteristics, the mean age of MMF and AZA groups were 42.2 and 35.4 yr, respectively, showing a significant difference (p=.015, Table 1). However, there were no significant differences in sex, underlying diseases, frequency of pretransplant PRA level (≥20%), HLA mismatching, cold ischemic time, donor and recipient's CMV serologic status and underlying disease, and ABO compatibility (Table 1).
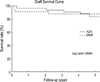
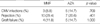
Treatment failure occurred in 12 patients (35.3%) of the MMF group by 6 months after transplantation, when compared with 11 patients (32.4%) in the AZA group without statistical significance (p>0.05). The frequency of clinical or biopsy-proven rejection treated with steroid pulse therapy were 29.4% and 20.6% in MMF and AZA groups, respectively (p>0.05). Two patients in MMF and one patient in AZA experienced graft loss during the 6-month follow up period, respectively. Death of one patient was reported in the MMF group during the same period. CMV infection was developed in 3 patients (8.8%) in the MMF group and 5 patients (14.7%) in the AZA group, not showing a significant difference (Table 2). One, three and five year graft survival rates were 91.1%, 88.2% and 88.2% in the MMF group and 97.1%, 94.1% and 83.1% in the AZA group, respectively (p>0.05) (Fig. 1).
DISCUSSION
The introduction of new immunosuppressive agents has significantly contributed to improve graft survival rate up to 90% in kidney transplantation. However, acute rejection is the most common cause of graft loss and a major factor influencing the long-term graft survival rate (1). As shown in several studies, in cadaveric renal transplantation, the major factors which influence the outcome of graft function are divided into immunologic factors and non-immunologic factors. Immunologic factors were reported to affect acute rejection, chronic rejection, and graft survival (2). Non-immunologic factors also should not be ignored because they are associated with delayed graft function, rejection, and graft survival (6, 7).
Several comparative studies have reported how immunosuppressive agents, which were developed to inhibit immunologic shade, have influenced acute rejection and graft survival. In particular, previously published data have indicated that MMF reduced acute rejection rate and improved graft survival during the early post-transplant period compared to AZA (5, 8). However, finding a study that considered the non-immunologic factors, especially donor factors is not easy. Thus, we designed a comparative case-control study to minimize the influence of donor factors by grafting the same cadaveric donor kidney.
Two kidney recipients grafted from the same cadaveric donor were randomized and assigned to either the MMF or AZA group. They received a triple immunosuppressive regimens, which consisted of CsA, prednisolon and either MMF or AZA according to the protocol, and their results such as acute rejection, graft survival and others were prospectively analyzed and compared. In summary, no difference was found in sex, HLA mismatching, weight, cold ischemic time, or underlying disease between the MMF and AZA group, while there was a significant difference in age factor. Recently data showed that censored graft survival-which excludes death with functioning graft-and the incidence of rejection episodes was equal in three adult groups of renal transplanted patients of different age (9). And a comparison of graft survival between children and elderly adults has been performed recently because recipient age may have an effect on renal graft survival due to its potential influence on the competence of the immune system. Though the incidence of acute rejections appeared to be significantly higher in the pediatric population, there was no significant difference in graft survival between both groups when death with functioning graft was excluded (10). So even though in our result there was significant difference in recipient age between two groups by univariate analysis, this result might be not meaningful because during this study the mean ages of both groups belong to low risk criteria due to above 18 yr old. There was no significant difference between the two groups in the incidence of acute rejection episodes and 5 yr graft survival rate. This is different from previous reports showing that MMF could reduce the incidence of acute rejection and improve graft survival.
Even though this study has some limitation of a small number of cases and relatively short-term follow up, these discrepant results might imply that donor factors could play an important role in cadaveric renal transplantation. Accordingly, donor factors deserve to be considered for the further clinical studies despite a small number of cases and a short follow-up period.

 XML Download
XML Download