

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Mechanical ventilation, the supportive therapy commonly used in respiratory failure, can cause lung injury and worsen outcome in acute respiratory distress syndrome (ARDS) patients (1). Recent research efforts in the ARDS focused on attempts to reduce mortality by limiting ventilator-induced lung injury (VILI) (2). Permissive hypercapnia is an inherent element of accepted protective lung ventilation, although such strategies may cause hypercapnic acidosis (3). Several research groups suggested that hypercapnic acidosis directly attenuates both primary (4-6) and secondary (7) ischemia-reperfusion-induced acute lung injury. Hypercapnic acidosis also directly protects against free radical-induced acute lung injury (4) and endotoxin-induced lung injury independent of ventilation strategy (8). In addition, hypercapnic acidosis attenuates lung injury induced by excessive lung stretch in both ex vivo (9) and in vivo (10, 11) models, by a surfactant independent mechanism (11). These findings suggested that hypercapnic acidosis per se may attenuate lung injury independent of ventilation strategies and that deliberate induction of hypercapnic acidosis by addition of CO2 to the inspired gas may have therapeutic potential in patients with ARDS (12, 13). However, hypercapnia may not be protective in all lung injury models. Rai et al. (14) demonstrated that hypercapnic acidosis does not appear to modulate the severity of VILI after surfactant depletion.
The present study was designed to investigate whether hypercapnic acidosis, induced by adding CO2 to inspired gas-modulates the development of VILI in normal rabbit model.
MATERIALS AND METHODS
Animals preparation and instrumentation
Care of the animals, techniques, and procedures were approved by the Animal Care and Use Committee of Chonnam National University Hospital. New Zealand white rabbits weighing 2.76±0.06 kg were anesthetized with an intramuscular injection of a ketamine hydrochloride (30 mg/kg) and xylazine (0.3 mg/kg). An endotracheal tube (3.5 mm internal diameter) was inserted via a tracheostomy. Mechanical ventilation was initiated in the pressure-controlled mode (IV-110B, Sechrist infant ventilator, Sechrist industries, Anaheim, CA, U.S.A.) with a peak inspiratory pressure (PIP) of 15 cm H2O, a positive end-expiratory pressure (PEEP) of 3 cm H2O, a frequency of 25 breaths/min, inspiration-to-expiration (I:E) ratio of 1:2 and an inspired oxygen fraction (FIO2) of 0.40. Anesthesia and paralysis were maintained throughout the experiment by continuous infusions of sodium pentobarbital (2-4 mg/kg/hr) and pancuronium bromide (0.03-0.07 mg/kg/hr). The internal carotid artery was cannulated with a 20-gauge catheter (Custom Product, Abbott Ireland, Sligo, Republic of Ireland) to monitor systemic arterial pressure and heart rate. Arterial blood gas samples were analyzed at 37℃ (Rapidlab 865, Chiron diagnostics corporation, U.K.) and corrected for body temperature. Rectal temperature was monitored and maintained within the range of 37±1℃ using a radiant heating lamp.
Experimental protocols
After recording baseline hemodynamic and gas exchange, 55 rabbits were randomly assigned to one of three groups (20 high pressure normocapnic group, 20 high pressure hypercapnic group, 15 control group). Control groups were ventilated with same baseline settings during the experiments (PIP of 15 cm H2O, PEEP of 3 cm H2O, I:E ratio of 1:2, and a FIO2 of 0.40). High pressure hypercapnic group (HPHC) was ventilated with PIP of 30 cm H2O, PEEP of 0 cm H2O and FIO2 of 0.40. Carbon dioxide was introduced into the inspiratory limb of the ventilator circuit, as necessary to maintain hypercapnia (PaCO2, 65 to 75 mmHg). High pressure normocapnic group (HPNC) was ventilated with same setting of HPHC, except normocapnia (PaCO2, 35 to 45 mmHg). Arterial blood gases were measured at every 1 hr during the experiment. Blood samples for lactate dehydrogenase (LDH) and aspartate aminotransferase (AST) were obtained at every 2 hr and measured by enzyme-linked immunosorbent assay (Olympus, AU 5400, Japan). After completion of the protocol, the heart-lung block was then removed after exsanguinations of the heparinized animals.
Bronchoalveolar lavage
The bronchoalveolar lavage fluid (BALF) was harvested from the right lung at the end of the experiment. Through the right mainstem bronchus, 35 mL of saline was infused slowly and withdrawn five times. The BALF was centrifuged and then divided into several aliquots to measure LDH, AST, and interleukin-8 (IL-8) concentrations. IL-8, a potent neutrophil attractant and activator, has been implicated in the neutrophil recruitment in lungs of patients with ARDS (15). Nakamura et al. (16) demonstrated that IL-8 level in BALF was increased and paralleled the BAL neutrophil counts during the lung injury. We examined the level of IL-8 in the BALF by enzyme-linked immunosorbent assay (ELISA).
Gravimetric analysis
Heparinization and exsanguinations were used to minimize the effect of residual blood on gravimetric indices. Left lung was physically sectioned into dorsal and ventral regions that were weighed separately to obtain wet weight (WW) and then desiccated in a vacuum oven at 60℃ to dryness for 4, 5 days until a constant dry weight (DW).
Histologic score
The resected lungs were infused with 4% paraformaldehyde solution from a tracheostomy tube. Subsequently, the trachea was clamped and the lungs were placed in 4% buffered paraformaldehyde solution. The lungs were divided into dorsal and ventral regions along a coronal plane connecting the mid-height caudal and cranial portions of the lungs. Subdivision into caudal and cranial sectors was accomplished by sectioning the lungs (in the transverse plane) along upper and lower lobe fissures. To avoid sampling bias, tissue samples of 3 µL were excised (regardless of macroscopic appearance) from the mid-portion of each sector. The samples were sectioned and stained (hematoxylin and eosin). The sections were later characterized using a semiquantitative grading system by a pathologist who was blinded as to the experimental protocol and region of sampling. After viewing approximately ten fields per sector under low and high power, each section was assigned a numerical histologic score ranging from 1 to 4, based on the degree of neutrophilic infiltration, hemorrhage, and edema in the interstitial and alveolar spaces as follows; 1 (normal), normal appearing lung; 2 (mild), minimal congestion, interstitial edema and interstitial neutrophilic infiltrate with occasional red blood cells and neutrophils in the alveolar spaces; 3 (moderate), moderate congestion and interstitial edema with neutrophils partially filling the alveolar spaces but without consolidation; 4 (severe), marked congestion and interstitial edema, with neutrophilic infiltrate nearly filling the alveolar spaces, or with frank lung consolidation. Atelectasis per se was disregarded and not scored as abnormality.
Statistical analysis
All values are reported as mean±standard deviation (SD), unless specified otherwise. Separate one-way analysis of variance (ANOVA) procedures were used to test for difference in variables. In each group, changes in measured variables over time were analyzed using a repeated-measures analysis of variance. A statistical package, SPSS 12.0 for Windows (SPSS Inc., Chicago, IL, U.S.A.), was used to analyze the data. A value of p<0.05 was considered significant.
RESULTS
Arterial CO2 tension and acid-base status
There were no significant differences in arterial carbon dioxide tension (PaCO2), and pH among the groups under baseline conditions. In the HPHC group, PaCO2 was increased and pH decreased quickly after the induction of carbon dioxide as compared with baseline values and then remained stable throughout the experiment. PaCO2 remained unchanged in the HPNC and control groups at each time point (Fig. 1A). In the HPNC and control groups, pH tended to be lower slowly throughout the experiment. However, there were no significant differences in pH from baseline values (Fig. 1B).
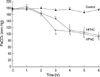
Changes in hemodynamics and arterial oxygenation
There were no significant differences in oxygenation and systemic arterial pressure among the groups under baseline conditions. In the HPHC and HPNC groups, systemic arterial pressure trended downward during the experiment as compared with control group. However, there were no significant differences in systemic arterial pressure between HPHC and HPNC group. In the HPHC and HPNC groups, PaO2 decreased progressively during the experiment. In the HPHC, PaO2 decreased significantly after 3 hr as compared with baseline values (171.6±7.9 vs. 113.4±12.1 mmHg; p<0.05). In the HPNC group, PaO2 decreased significantly after 4 hr as compared with baseline values (173.5±11.6 vs. 112.3±11.7 mmHg; p<0.05). At the end of the protocol, however, there was no significant difference in oxygenation between HPHC and HPNC groups (Fig. 2).
Serum levels of AST and LDH
Serum levels of AST and LDH elevated progressively during the experiments in injurious ventilator patterns (HPHC and HPNC groups) when compared with the control group. There were no significant differences of serum levels of AST and LDH between HPHC and HPNC groups at each time point (Fig. 3). In the control group, the trend toward elevated levels of AST and LDH over time was not statistically significant when compared with baseline values.
BALF levels of AST, LDH, and IL-8
The levels of LDH, AST and IL-8 in the BALF, measured at the end of the experimental period, were significantly higher in the HPHC and HPNC groups when compared with the control group (p<0.05) (Fig. 4). There were no significant difference in BALF LDH, AST, and IL-8 levels between HPHC and HPNC group.
Gravimetrics
The ratio of wet weight to dry weight (WW/DW) for dependent and nondependent regions was significantly greater in injurious ventilatory pattern (HPHC and HPNC group) than the control group. The WW/DW for dependent regions was highest in the HPHC, intermediate in the HPNC, and lowest in the control group (HPHC: 7.88±1.52; HPNC: 7.42±1.25; control: 5.09±0.47; p<0.05). There were no significant difference in WW/DW for dependent regions between HPHC and HPNC group. The WW/DW for nondependent regions was also the highest in the HPHC, intermediate in the HPNC, and lowest in the control group (HPHC: 6.12±0.97; HPNC: 5.84±1.17; control: 4.21±0.29; p<0.05). There were no significant difference in WW/DW for nondependent regions between HPHC and HPNC group (Fig. 5).
Histology
Gross postmortem inspection of the lungs in the HPHC and HPNC group revealed edema and hemorrhage that were most prominent in the dependent regions. Histologic scores for dependent and nondependent regions were significantly higher in injurious ventilator patterns (HPNC and HPHC group) than the control group. However, no significant differences was found in histologic scores for dependent and non-1HPHC and HPNC group (Fig. 6).
DISCUSSION
The principal finding of this study was that hypercapnic acidosis (induced by direct administration of CO2) could not reduce VILI arising from high-pressure mechanical ventilation. Oxygenation and hemodynamic changes in the HPHC and HPNC groups were very similar throughout the study. Based on the inflammatory response in the BAL fluid, WW/DW, and histologic scores, our data demonstrate that hypercapnic acidosis, induced by CO2 insufflation, does not decrease the severity of VILI in this model.
Protective ventilatory strategies that involve hypoventilation result in both limitation of tidal volume and elevation of systemic carbon dioxide tension. Such "permissive hypercapnia" may be associated with increased survival in ARDS (3). The importance of alterations in CO2 tension in critical care is increasingly recognized (13). Hypercapnia results in a complex interaction between altered cardiac output, hypoxic pulmonary vasoconstriction, and intrapulmonary shunt, with a net increase in arterial oxygenation (17). Acidosis may reduce cellular respiration and oxygen consumption (18), which may further benefit an imbalance between supply and demand, in addition to greater oxygen delivery. Although hypercapnic acidosis exerts biologically important beneficial effects in various experimental models (4-11), there are concerns regarding the potential for hypercapnic acidosis to exert deleterious effects that suggest the need for caution when considering its use in the clinical settings.
In VILI, Ranieri et al. (19) demonstrated that the concentrations of proinflammatory cytokines in both bronchoalveolar lavage and plasma could indeed be decreased in patients ventilated with a lung-protective strategy. A report showed that serum aspartate aminotransferase and LDH were significantly higher in the positive pressure ventilation with overdistension of the lungs compared with the control group (20). Our results showed that serum levels of AST and LDH elevated progressively during the experiments in injurious ventilator patterns (HPHC and HPNC groups) when compared with the control group. There were no significant differences of serum levels of AST and LDH between HPHC and HPNC groups at each time point.
Broccard and colleagues (9) demonstrated that BALF protein concentration and WW/DW ratio was higher in the HPNC than in the HPHC group. Sinclair et al. (10) demonstrated that eucapnic group showed significantly higher plateau pressures, WW/DW ratio, BALF protein concentration, and injury score. These findings suggested that hypercapnic acidosis decreased the severity of VILI. However, our results showed that there were no significant differences of the levels of BALF AST, LDH, and IL-8 between HPHC and HPNC group. Our results also demonstrated that WW/DW and histologic scores did not differ between HPHC and HPNC group. Based on our results, we suggest that hypercapnic acidosis at least induced by CO2 insufflation might not be considered as a protective effect against VILI in this model.
Despite these unique results, this study has limitations in its application to the practical clinical use. First, Broccard et al. (9) and Sinclair et al. (10) maintained PaCO2 between 70 and 100 mmHg, but the target PaCO2 in this study was between 65 to 75 mmHg. The optimal degree of hypercapnia for potential use in critically ill patients is unknown, as well as potential interactions with other therapies and specific contraindications (8). Second, whether hypercapnia resulting from hypoventilation and hypercapnia resulting from inhaled CO2 may provide equivalent lung protection is still unknown. Many of critically ill patients have underlying chronic illness and acute organ dysfunction that may limit their tolerance and ability to compensate against hypercapnia (21) and there are no long-term clinical outcome data to support the practice of therapeutic hypercapnic acidosis (22). In conclusion, our data suggest that hypercapnic acidosis resulting from direct administration of CO2 may not be a useful therapeutic intervention in VILI.





 XML Download
XML Download