

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The stunned myocardium, a reperfused myocardium after brief ischemic episodes, exhibits a prolonged impairment of systolic as well as diastolic function, despite the absence of cell necrosis (1). The myocardial stunning usually recovers spontaneously and requires no therapy. However, if the stunning is severe or involves parts of the left ventricle large enough to cause impairment of global ventricular function, it can be reversed with several inotropic agents, such as dobutamine, epinephrine, amrinone, a phosphodiesterase III inhibitor, and calcium chloride (CaCl2) (2-4).
A transient myocardial ischemia may induce a marked endothelial dysfunction, which results in decreased coronary flow reserve and vasodilator responsiveness (5-7). Furthermore, the postischemic myocardium shows normal oxygen consumption (MVO2), despite the depressed contractile function, i.e., increased oxygen cost of contractility (8). In this context, inotropic drugs may alter coronary vascular responses and hence affect myocardial oxygen balance in stunned myocardium. A previous study indeed demonstrated in postischemic canine myocardium that mechanical function was not as tightly coupled as coronary blood flow (CBF) and MVO2, and thus oxygen extraction (EO2) was rather increased during inotropic stimulation with dobutamine (9).
It has been also demonstrated that ischemia and reperfusion injury may dampen inotropic responses to β-adrenergic stimulation (10). Moreover, an intracellular Ca2+ overloading during ischemia and reperfusion has been implicated in the pathogenesis of myocardial stunning (11). Since dobutamine and epinephrine exhibit their inotropic activity through β-adrenergic stimulation to increase intracellular Ca2+ availability, their inotropic potency may be diminished in postischemic myocardium. On the contrary, the inotropic activity of amrinone may not be similarly affected. Furthermore, administration of CaCl2 may augment calcium overload and deteriorate the regional function in postischemic myocardium. The present study was aimed to determine the effects of dobutamine, epinephrine, amrinone, and CaCl2 on regional oxygen balance and mechanical function in postischemic stunned myocardium.
MATERIALS AND METHODS
The study was approved by the Institutional Review Board of Experimental Animal Research. Mongrel dogs of either sex, weighing 17-35 kg, were anesthetized with an intravenous bolus of thiopental sodium (10-15 mg/kg). After tracheal intubation, anesthesia was maintained with halothane (1.0% end-tidal; Datex, Helsinki, Finland) in 100% oxygen via positive pressure ventilation. Tidal volume and respiratory rate were adjusted to maintain the end-tidal CO2 concentration of 4.5-5.5%. To obtain muscular relaxation, vecuronium bromide was used (0.1 mg/kg as a bolus, followed by a continuous infusion at 0.05 mg/kg/h). Body temperature and electrocardiogram were continuously monitored. Ringer's lactate solution was intravenously administered (5 mL/kg/hr).
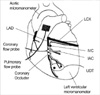
A left thoracotomy was performed via the fifth intercostal space to suspend the heart in a pericardial cradle. The instruments were implanted in and around the heart as shown in Fig. 1. Doppler transit time flow probe (Transonic System Inc., Ithaca, NY, U.S.A.) was placed around the main pulmonary artery for measurement of cardiac output, and another flow probe was placed around the left anterior descending coronary artery (LAD) just distal to the first diagonal branch for continuous blood flow measurement. A rubber band was placed around LAD immediately distal to the flow probe to serve as an occluder. For the infusion of drugs, a 24-gauge catheter was inserted into the proximal LAD. A pair of ultrasonic dimension transducers (Medical Research Technology, Gaithersburg, MD, U.S.A.) was implanted approximately 10 mm apart in the subendocardium of the anterior wall that demonstrated cyanosis during a brief test occlusion of LAD. A catheter-tipped micromanometer (SPR-524, Millar Instruments, Houston, TX, U.S.A.) was inserted directly into the left ventricle via an apical incision for measurement of left ventricular pressure (LVP). The first derivative of LV pressure (dP/dtmax and -dP/dtmin) was obtained by electronic differentiation.
The right femoral artery was cannulated for measurement of aortic pressure with a catheter-tipped micromanometer and for blood sampling. An 18-gauge catheter was inserted into the left atrium for the measurement of luminal pressure (Datex, Helsinki, Finland), and a 24-gauge catheter into the anterior interventricular vein at the same level as the LAD occluder for measurement of coronary venous oxygen and lactate concentrations (12).
Oxygen (Gem Premier; Instrumentation Laboratory, Lexington, MS, U.S.A.) and lactate concentrations (Vitros 950; Ortho-Clinical Diagnostics, Rochester, NY, U.S.A.) were measured in blood drawn simultaneously from the coronary vein and artery. MVO2 of the anterior myocardial wall was calculated by multiplying the arteriovenous oxygen difference by total LAD flow. EO2 or myocardial lactate extraction (Elac) (in percent) was calculated by dividing the arteriovenous difference by the arterial content. Plasma Ca2+ concentrations were also measured from the anterior interventricular venous blood using blood gas analyzer (Gem Premier; Instrumentation Laboratory, Lexington, MS, U.S.A.).
Experimental protocol
After a sufficient stabilization period of 60 min, pre-infusion mechanical and hemodynamic data were collected. Simultaneous measurements of arterial and coronary venous oxygen and lactate contents (metabolic data) were made. The animals then received intracoronary infusions of either dobutamine (n=11; 0.05, 0.125, and 0.375 µg/mL CBF), epinephrine (n=10; 0.004, 0.01, and 0.03 µg/mL), amrinone (n=10; 2, 5, and 10 µg/mL), or CaCl2 (n=11; 0.10, 0.25, and 0.75 mg/mL) with a syringe pump (STC 524, Terumo, Japan). The concentration ranges for dobutamine, amrinone, and CaCl2 were selected because they have been shown previously to produce a comparable dose-dependent increase of %SS when given intracoronarily in normal myocardium (2, 13). The range of epinephrine had been demonstrated in pilot studies to cause an increase of %SS comparable with that observed during dobutamine infusion. The blood concentrations for each inotropic agent examined include the clinical dose range (dobutamine, 0.1-0.2 µg/mL; amrinone 2-7 µg/mL) (14, 15). Each inotropic drug was infused for 3 to 5 min in incremental doses administered 8 to 10 min apart each. Measurements were made at the end of each dose, and the mechanical data were obtained 5 min after each dose. Following one series of experiment in normal myocardium, a 15-min LAD occlusion and subsequent reperfusion were made to stun the myocardium, as described by previous investigators (2, 7). Approximately 30 min after the onset of reperfusion, when hemodynamic and flow values were stable, the same infusion protocol in each group was repeated. Inotropic drugs were infused at 0.3-2.0 mL/min. The intracoronary infusion rate of inotropic drug was calculated by multiplying the desired coronary blood concentration by LAD flow rate.
Data acquisition and analysis
Blood flows, segmental dimension of anterior wall, and LV and mean aortic pressures were continuously monitored. End-systolic segment length (ESL) was determined at the point approximately 20 msec before peak negative LV dP/dtmin, and end-diastolic segment length (EDL) was determined at the onset of left ventricular isovolumetric contraction (16). Regional myocardial contractility was determined using percent segment shortening (%SS, [(EDL-ESL)/EDL]×100). Percent post-systolic shortening (%PSS) as a regional diastolic function was calculated by [(LminD-ESL)/(EDL-LminD)]×100, where LminD=minimum length during diastole. Coronary perfusion pressure was calculated by the difference of left atrial pressure from aortic diastolic pressure.
At the end of the experiment, the heart was stopped by intra-atrial injection of concentrated potassium chloride solution. The area supplied by LAD artery was defined by injection of Evans blue into the vessel at the site of the flow transducer. Careful weighing of the stained muscle allowed mean flow to be calibrated in mL/min per 100 g of muscle. The LAD perfusion territory was 27.6±6.2% of total left ventricular mass.
Statistical analysis
All data are presented as mean±SD. Statistical analysis of the data was performed by two-way analysis of variance (ANOVA) for repeated measures followed by Dunnett's t test. Comparisons between normal and stunned myocardium were made by paired Student's t-test. Significance was assumed when p<0.05.
RESULTS
Of the 58 animals instrumented, eight were excluded from data analysis because of pre-ischemic lactate production. One of 12 animals given dobutamine, 2 of 12 given epinephrine, 2 of 12 given amrinone, and 3 of 14 given CaCl2 died due to ventricular fibrillation during coronary occlusion or immediately after the onset of reperfusion. They were also excluded.
Global ventricular function
Table 1 shows systemic hemodynamic variables obtained before and during intracoronary infusion of inotropic drugs. Neither drugs significantly affected these variables in normal myocardium, except for increases in dP/dtmax. LAD occlusion slightly increased heart rate and left atrial pressure, and decreased mean aortic pressure, dP/dtmax, dP/dtmin, and cardiac index. They quickly returned toward the baseline values with the onset of reperfusion, except dP/dtmax and -dP/dtmin, which were kept lower than their preocclusion baseline values. In stunned myocardium, the effects of inotropic drugs were similar to those in normal myocardium.
Regional ventricular function
Table 2 shows the regional mechanical function in normal and stunned myocardium. All inotropic drugs examined caused dose-dependent increases in %SS and decreases in ESL, while they did not affect %PSS, in normal myocardium. LAD occlusion rapidly increased EDL (10.0 to 10.8-10.9) and %PSS (2-5% to 72-79%), with systolic bulging apparent within 1-3 min. Subsequent reperfusion produced a transient increase in %SS followed by a gradual decline to 7.4-9.0% (44-51% of preischemic baseline values) at 30 min of reperfusion, which did not differ between the groups. In stunned myocardium, however, inotropic drugs resulted in changes similar to those in normal myocardium, except for a progressive reduction of %PSS. When inotropic drugs were stopped, %SS returned rapidly toward, but not below, their postischemic baseline values in stunned myocardium (data not shown).
Coronary blood flow and oxidative metabolism
Table 3 shows the effects of inotropic drugs on MVO2, CBF, and EO2 in normal and stunned myocardium. The inotropic drugs in normal myocardium caused dose-dependent increases in MVO2 and CBF. However, with epinephrine and amrinone, CBF increased more markedly than did MVO2, resulting in decreases in EO2 and increases in PvO2, whereas it increased in parallel with those of MVO2 with dobutamine and CaCl2, resulting in EO2 and PvO2 unaltered (Fig. 2). After LAD occlusion and reperfusion, CBF was not significantly affected and MVO2 was slightly decreased from baseline values of normal myocardium, despite the severely impaired contractile function. However, neither metabolic nor CBF responses to inotropic drugs were significantly affected except that epinephrine caused proportional increases in CBF relative to MVO2, resulting in EO2 and PvO2 unaltered in the stunned myocardium. Although significantly reduced by the ischemia and reperfusion insult itself, Elac was not affected by inotropic agents, except for that epinephrine caused a decrease in stunned myocardium (Fig. 3). Plasma Ca2+ concentrations in the coronary vein increased dose-dependently in normal and stunned myocardium in the CaCl2 group (data not shown).
DISCUSSION
The present study showed that the inotropic drugs examined improved the regional systolic and diastolic functions in stunned myocardium. Coronary vasodilator responses to inotropic drugs were well maintained, although a direct vasodilator response to epinephrine was abolished. Percent segmental shortening returned to the postischemic baseline values after discontinuation of inotropic drugs. Furthermore, the myocardial contractile responses to the inotropic drugs were not altered. These findings are in accord with those in previous studies which also demonstrated a normal contractile reserve in response to inotropic stimulation in stunned myocardium (2, 3). Taken together, a brief myocardial ischemic insult may not significantly affect either β-adrenergic signaling pathway or contractile response to Ca2+. In particular, inotropic drugs including CaCl2, acting through an increase in intracellular Ca2+ availability, are unlikely to deteriorate mechanical function in the stunned myocardium, although Ca2+ overloading is causally related with the pathogenesis of myocardial stunning (11). In fact, viable cells regain control of cytoplasmic Ca2+ very rapidly after ischemia and hence intracellular Ca2+ levels return to a baseline value after 20 min of reperfusion (17).
Although effects of inotropic drugs on the systolic function have been extensively studied in the stunned myocardium, little information has been available about their effects on diastolic function. In the present study, the drugs examined did not affect peak -dP/dtmin but produced a progressive reduction of %PSS, a sensitive index of myocardial ischemia (18). Schlack et al. (19) similarly observed that intracoronary norepinephrine did not affect peak -dP/dtmin but reduced post-ejection wall thickening in an open chest canine model. The drugs may have improved early diastolic function. On the other hand, peak -dP/dtmin has been demonstrated to reflect ischemia-induced changes in contractility (i.e., peak ventricular pressure) rather than relaxation in regionally ischemic canine hearts in an open chest canine model (20). The unaffected aortic pressure during the infusion of inotropic drugs in the present study may be related to unaltered peak -dP/dtmin.
The reduced contractile function in stunned myocardium has been associated with an unaltered MVO2 (8). If the contractile function increases at a higher energy cost in stunned myocardium, one would expect an elevated CBF for a given level of contractility (assuming an unchanged EO2). However, the present study showed that CBF in relation to segment shortening was comparable in normal and stunned myocardium. Chiu et al. (21) have demonstrated that regional inotropic stimulation with isoproterenol restores synchrony and regional work in stunned myocardium, without greatly affecting regional MVO2 in dogs. They speculated that the myocardial stunning produced asynchrony between force development and segment shortening, thereby decreasing systolic regional work (but not total work) to a greater extent than MVO2. It is likely that inotropic drugs do not increase total mechanical work but reclaim the synchrony. They may not cause greater increases in CBF relative to regional work in stunned myocardium.
An endothelial dysfunction has been demonstrated after a brief ischemic episode (5-7). However, in the present study, the degree of CBF increases in response to inotropic drugs did not differ between the normal and stunned myocardium, with the exception of epinephrine which increased CBF in parallel with MVO2. Buffington and Rothfield (3) similarly observed an appropriate increase of CBF when regional contraction was stimulated by CaCl2 in stunned porcine myocardium. Taken together, in stunned myocardium, inotropic drugs do not interfere with normal metabolic vasoregulation, by which CBF is maintained in proportion to the myocardial oxygen demand. It is unlikely that the inotropic drugs directly affect coronary vascular tone even after a brief ischemic insult.
Nitric oxide (NO) has been known to mediate β-adrenergic dilation of resistance coronary vessels in dogs (22), and peripheral vasodilation induced by amrinone in rat thoracic aorta (23). Although EO2 was progressively decreased by epinephrine in normal myocardium, it was unchanged in stunned myocardium, suggesting that an ischemic insult abolished its vasodilator effect (Fig. 2). It has been shown that endothelium-dependent vasodilation involving NO is impaired in stunned coronary endothelium (7). The abolished vasodilator effect of epinephrine may be related to a diminished NO production. In contrast, amrinone increased CBF in stunned myocardium, the degree of which did not differ from that in normal myocardium. Amrinone causes vasodilation in part via release of endothelium-derived NO in rat thoracic aorta (23). The maintenance of direct vasodilator response in stunned myocardium may then indicate that NO does not mediate the amrinone-induced vasodilation in coronary circulation.
Myocardial lactate extraction was progressively decreased with increasing doses of epinephrine in stunned myocardium in the present study, suggesting an anaerobic metabolism (Fig. 3). Stahl et al. (24) observed an increased heterogeneity of oxygen extraction with very low venous oxygen saturation in stunned myocardium despite patent microvasculature and normal perfusion, implying either focally impaired perfusion or increased metabolic activity. Epinephrine may have caused focal microcirculatory changes with localized areas of tissue hypoxia and anaerobic metabolism, despite the unaltered coronary venous oxygen tension. However, lactate production was more pronounced with epinephrine than with other three drugs, despite comparable increases in MVO2 and CBF, in stunned myocardium. It is unlikely that the impaired myocardial perfusion appreciably limited oxidative metabolism during epinephrine infusion. One more likely explanation may include the metabolic effect of epinephrine on glucose. Totaro and Raper (25) observed that after cardiopulmonary bypass epinephrine causes systemic lactic acidosis in some patients without apparent tissue ischemia. They speculated that epinephrine inhibited pyruvate dehydrogenase through β-2 adrenoceptor agonistic effects and thus pyruvate shunted toward lactate to preserve intracellular energy supply. It is suggested that epinephrine may have impaired pyruvate metabolism, resulting in an increased lactic acid production in stunned myocardium.
There are several limitations in the present study. First, halothane, instead of pentobarbital that has no direct coronary or myocardial effect, was used to maintain anesthesia during the study. Volatile anesthetics have been shown to enhance recovery of postischemic myocardium (26). Halothane may have some protective effects against ischemia and reperfusion injury of the myocardium and therefore altered the response to inotropic drugs. In addition, volatile anesthetics have been shown to directly produce coronary vasodilation in vivo (27). However, it has been demonstrated that responses to inotropic drugs under halothane anesthesia do not differ from those under fentanyl-midazolam anesthesia in postischemic myocardium in dogs (28). Second, in the present study, inotropic drugs were administered before and after LAD occlusion. CaCl2 and phosphodiesterase III inhibitor (i.e., amrinone) have been demonstrated to precondition myocardium against postischemic contractile dysfunction (29). CaCl2 or amrinone administered before LAD occlusion may have then altered its contractile responsiveness of postischemic myocardium. However, the responses to CaCl2 in stunned myocardium were similar regardless of whether it was administered before LAD occlusion or not, indicating that preconditioning effects of CaCl2 are minor or null. Third, the time course of recovery of postischemic, reperfused myocardium was not evaluated to verify the constancy of regional segment shortening in the previously ischemic zone during the time period corresponding to drug infusion (30-70 min of reperfusion). However, regional contractile function (%SS) remained constant between 30 and 90 min of reperfusion in an openchest canine model similar to ours (30). Furthermore, %SS returned to the preinfusion baseline level after cessation of inotropic drug infusion. Finally, heart rate and systemic blood pressure (coronary perfusion pressure) were not controlled during the study. Changes in these systemic hemodynamic variables during infusion of inotropic drugs may increase MVO2 and CBF. However, neither drug affected aortic pressure, heart rate, and coronary perfusion pressure throughout the study.
In conclusion, the inotropic drugs examined improved the regional systolic and diastolic functions in the postischemic stunned myocardium in a dose-dependent manner, as was in the normal myocardium. The enhanced regional functions were accompanied by increases in CBF, which were not affected by an ischemia and reperfusion insult, except for an abolition of direct coronary vasodilator effect of epinephrine.





 XML Download
XML Download