

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Plasmodium vivax, the causative agent of vivax malaria, is the second most common species of malaria with a yearly estimate of 35 million cases worldwide (1). Prior to the 1970's when the Republic of Korea (ROK) was determined to be "malaria free", vivax malaria was a significant civilian and military public health threat (2-4). During the Korean War (1950-1953), the ROK and U.S. military suffered many casualties as a result of vivax malaria. For example, approximately 15% of all febrile illnesses among ROK military personnel were due to malaria (2-5). With the initial use of chloroquine, U.S. casualties in the ROK were decreased, but cases soon showed up in the U.S. as a result of hypnozoites. The discovery of primaquine and its use soon reduced malaria casualties among U.S. soldiers throughout the remainder of the war (6). Even so, during 1953 at the end of the war, more than 3,000 U.S. soldiers and nearly 9,000 ROK Army soldiers were diagnosed with malaria (7). Following the signing of the armistice and reduced hostilities in 1954, malaria cases decreased to fewer than 6,000 among ROK Army soldiers (8). As socioeconomic conditions in the ROK improved and associated malaria control efforts were strengthened, the ROK was declared "malaria free" in 1979 (4). However, focal indigenous cases continued to be reported through 1984 (9).
It was not until 1993 that vivax malaria returned with a vengeance along the demilitarized zone (DMZ), increasing exponentially through 2000 (4,142 cases), and only decreasing through 2002 as a result of an extensive chemoprophylaxis program instituted by the ROK Army among combat units assigned to "high-risk" areas near the DMZ (10-14).
Almost all of the re-emerging malaria cases have been confined to the northern part of Gyeonggi Province and the north-western part of Gangwon Province near the DMZ, where large numbers of soldiers are stationed. Because of this geographical distribution and exposure of personnel during training/operations, most cases were reported among soldiers since the beginning of the epidemic. To cope with the exponentially increasing malaria rates among various military units, chemoprophylaxis (chloroquine followed with terminal primaquine) was initiated among military personnel assigned to "malaria high-risk areas" in 1997 in an attempt to reduce malaria rates among soldiers and spread to civilian populations throughout the ROK. The chemoprophylaxis program was expanded annually from approximately 16,000 (1997) to more than 140,000 in 2002. Decreased numbers of malaria cases experienced by the ROK Army were attributed to the annual expansion of chemoprophylaxis in "high-risk" malaria areas, especially since 1999 (12). While mass chemoprophylaxis was used on a large scale among U.S. soldiers during the Korean War, the use of large-scale chemoprophylaxis in the ROK Army is unprecedented. Therefore, an evaluation of the effectiveness of the chemoprophylaxis program is required not only to determine its effect on the reduction of malaria cases, but also to monitor for increased parasite tolerance/resistance to chloroquine and/or primaquine. In this study, we evaluated the effects of disease reduction of mass chemoprophylaxis for selected ROK Army units, i.e., monthly and annual incidence, geographic dispersion and direct comparison on the number of malaria cases of neighboring units.
MATERIALS AND METHODS
Malaria, defined as, any febrile illness and demonstration of P. vivax parasites in peripheral blood smears, is a reportable disease to the Ministry of Health and Welfare, ROK (4, 15). All malaria cases among ROK military personnel are reported to the Office of the Surgeon General, Army Headquarters, to the Ministry of Health and Welfare. All cases of vivax malaria that were reported to the Korean Ministry of National Defense from 1 January 1993 through 31 December 2002 were reviewed and their epidemiological characteristics, e.g., date of disease onset, status of receiving chemoprophylaxis and location of their service unit, analyzed.
Malaria case data among ROK military veterans (most after serving 26 months) and civilians were acquired from the Department of Epidemiology, National Institute of Health (Seoul, Republic of Korea). Cases among military veterans were defined as those who 1) developed malaria within 24 months after discharge from military service, and 2) had been stationed during their military services in a malaria-risk area. Otherwise, veterans were reported as civilians. All of the cases defined here as "military veterans" were excluded from this study since most did not complete terminal primaquine prophylaxis in the year that they were discharged from military service. "Malaria-risk" areas were reported during the preceding year(s) as those areas where malaria cases were reported. Epidemiologic characteristic data from civilians were compared with the data from ROK military personnel.
To evaluate the effects of mass chemoprophylaxis, we identified paired military units (chemoprophylaxis and no chemoprophylaxis) located within a 1.5-kilometer radius, and similar levels of malaria prevalence and socio-behavioral conditions. Also, we analyzed the occurrence of malaria cases between neighboring units during the same periods. Data for each unit, including the unit branch, location, the number of soldiers, and training situation, were obtained through interviews with corresponding unit medical officers. Soldiers received weekly oral 400 mg-hydroxychloroquine sulfate (Haloxin™, Han Lim Pharmaceutical Co., Republic of Korea, Aruquin™, Unimed Pharmaceutical Inc., Republic of Korea, Rumaqin™, Hana Pharmaceutical Co., Republic of Korea) from June through early October followed by daily oral 15 mg-primaquine phosphate (Praquine™, Daewoo Pharmaceutical Co., Republic of Korea, Malaquin™, Ahn Gook Pharmaceutical Co., Republic of Korea) for two weeks. Test for glucose-6-phosphate deficiency before primaquine prophylaxis was not done because it is very rare in Koreans.
The statistical analysis for the data was done with SAS version 8.0 (SAS Institute Inc., Cary, North Carolina, U.S.A.). Comparisons of malaria incidence between treatment and control groups were made by Mantel-Haenszel χ2-test. The primary efficacy parameter was based on malaria rates of the paired treatment and control groups, such that: efficacy of chemoprophylaxis=1-[(rate of disease among the chloroquine/primaquine treatment group)/(rate of disease among the control group)].
RESULTS
The ROK Army initiated chemoprophylaxis to nearly 16,000 soldiers in 1997 (Table 1). The numbers of soldiers administered chemoprophylaxis increased thereafter until more than 140,000 soldiers were provided chemoprophylaxis by 2002. The prophylactic schedule was initiated about mid-June in 1997. In subsequent years, malaria chemoprophylaxis was initiated during the 1st and 2nd weeks of June until 2000. During 2001 and 2002, it was initiated during the 2nd week of May.
Prior to the initiation of chemoprophylaxis, the ROK Army accounted for >80% of all malaria cases (Table 2). With the introduction of chemoprophylaxis in 1997 and subsequent years, the proportion of military cases accounted for 67% (1997) to 24% (2002). During 1999 through 2002, a decrease in malaria incidence in the military occurred approximately 1-2 weeks after the chemoprophylaxis schedule was initiated in early June or in mid-May (Fig. 1). This was inconsistent with the steady increase of malaria cases among civilian populations that were not provided chemoprophylaxis. The proportion of annual cases among military members for the period when chemoprophylaxis was initiated to one week after the final dose of chloroquine during 1999 through 2002 was 71% (771/1,085), 75% (960/1,288), 82% (550/673) and 80% (338/425) of the total annual number of cases, respectively. On the other hand, the proportion of annual malaria cases among civilian populations was 87% (1,337/1,541) in 1999, 88% (1,333/1,515) in 2000, 87% (963/1,112) in 2001 and 88% (760/864) in 2002 during this same period.
Through 1997, more than 90% of the total military cases occurred in areas of highest prevalence including Yeoncheon, Paju, and Cheolwon Counties where chemoprophylaxis was provided at the early stage. Case occurrences in these regions gradually decreased to 56% by 2002 (Table 2).
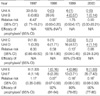
Risk factors for the potential exposure to infected anopheline mosquitoes, including geographic and socio-behavioral for ROK Army units are shown in Table 3. The occurrence of malaria among paired units is shown in Table 4. Units A and B were infantry units located in Paju County approximately 3 km from the DMZ and with missions to patrol activity along the DMZ. Due to its higher malarial rates in 1997, Unit A was provided chemoprophylaxis from 1998 through 2000. Chemoprophylaxis was initiated for Unit B in 1999 when malaria rates reached 4%.
Units C and D were similarly located in Paju County. Unit C and D were approximately 4 km and 4.5 km from the DMZ, respectively. Unit C (infantry unit) had more frequent field and night training missions than Unit D (artillery unit). Chemoprophylaxis was initiated in Unit C in 1999 and in Unit D in 2000. The incidence of malaria was similar between these groups in 1997 and 1998 (p>0.05) but the incidence was significantly lower in the unit C in 1999 (p<0.001). In 1999, when chemoprophylaxis was initiated, malaria incidence of Unit C was less than one-seventh of that of Unit D in spite of greater potential of exposure to the vector populations (Table 4).
Units E and F were located within 2 km of each other in Cheolwon County, approximately 4 km from the DMZ. Chemoprophylaxis was initiated in Unit E in 1998 but was not performed in Unit F. Units E and F showed no significant difference in the incidence of malaria in 1997 (p>0.05). All ROK Army units given chemoprophylaxis demonstrated significantly lower incidence rates of malaria when compared to untreated units (p>0.05). The efficacy of chemoprophylaxis, based on malaria rates among treated and untreated units, ranged 80-100%.
DISCUSSION
Vivax malaria in Korea is characterized as unstable malaria, e.g., low rates of disease with occasional local epidemics due to environmental factors, topography, agricultural change (reduction of livestock in North Korea), inefficient vector control, and political and socioeconomic factors (17). Additional factors contributing to the instability of malaria transmission in the ROK include a short transmission season (May through October) and high vector populations (17).
Since its re-emergence in 1993, malaria cases had grown exponentially through 1997 (11, 12). During this period, more than 80% of the total number of annual cases occurred in the ROK military, including veterans, and almost all of them were assigned to units located near the DMZ (11, 12). This resulted in a major health threat that the Korean Ministry of National Defense had to address, in addition to the spread of malaria from military to civilian populations south of the DMZ as veterans and travelers exposed to malaria in endemic regions returned home. In 1997, the Korean Ministry of National Defense addressed the increasing numbers and spread of malaria throughout the ROK, in part, by initiating a chemoprophylaxis policy using chloroquine and primaquine. Soldiers received weekly oral 400 mg-hydroxychloroquine sulfate from June through early October followed by daily oral 15 mg-primaquine phosphate for two weeks (18-22).
Compliance in any mass chemoprophylaxis program that covers large populations is a major issue. While it was recommended that military commanders and their staffs ensure that all soldiers take chloroquine under direct observation, some units failed to comply with this recommendation (8). Thus, soldiers that contracted malaria in areas where chemoprophylaxis was provided may not have taken chloroquine as directed. However, other factors that were not evaluated, e.g., incomplete absorption of the drug or drugs that have lost their potency due to inappropriate storage or expiration may have resulted in some cases. Additionally, parasites may develop a tolerance/resistance to blood concentrations of chloroquine in persons on chemoprophylaxis, creating an additional burden on the public health system to use other more expensive anti-malarial drugs or increase treatment regimens. These factors must be considered and monitored whenever mass chemoprophylaxis is planned or initiated to ensure a safe and effective program. Since blood concentrations of chloroquine were not determined for soldiers on chemoprophylaxis, there is no evidence that the strains of vivax malaria circulating in the ROK are tolerant/resistant to chloroquine therapy.
Even though there were malaria cases among the "treatment groups" (chemoprophylaxis), they demonstrated a significant reduction from the previous years while their paired "control groups" (no chemoprophylaxis) increased significantly (12). We can find this phenomenon in Table 4. Even though Units D and F had less exposure than their paired units, malaria greatly increased in these units when not provided chemoprophylaxis while decreasing in their paired units when they were given chemoprophylaxis. These results also demonstrate that even with partial chemoprophylaxis in malaria "high-risk" areas, malaria rates decreased while expanding in adjacent counties where chemoprophylaxis was not provided. The positive effect in the reduction of malaria cases is further supported by evidence that when chemoprophylaxis was initiated, at about a one-week interval, malaria cases were reduced in military populations, while they continued to increase among civilian populations. Had the intervention of chemoprophylaxis not been instituted, it is assumed, based on civilian data, that the malaria rates in the military populations would have been much greater. If chemoprophylaxis was not performed in the military, malaria cases might have increased mainly during the prophylactic period, and it resulted in similar proportion of malaria among military personnel for prophylactic period with that among civilian populations for same period. This also would have an impact on the number of civilian/veteran cases by reducing secondary transmission of the "prevented" cases. Overall reduction in malaria cases in ROK Army might have been even greater if soldiers had taken chloroquine completely as directed. But due to poor compliance in some soldiers, malaria cases reported.
Previous U.S. experiences during the Korean War demonstrated that large numbers of casualties as a result of malaria were successfully reduced when mass chemoprophylaxis, using chloroquine and later with terminal primaquine was applied (5). Thus, historically the use of chemoprophylaxis in Korea effectively reduced the malaria threat under wartime conditions. Chloroquine usage continues to be the recommended prophylactic regimen against vivax malaria where there is no chloroquine-resistant parasites (18-22). Chemoprophylaxis with chloroquine and primaquine on a large scale in the ROK Army to reduce vivax malaria casualties provides an opportunity to evaluate the effect of mass chloroquine/primaquine prophylaxis during armistice conditions (23).
Results described herein show that chemoprophylaxis used in high-risk malaria areas is at least one of the factors that reduced malaria rates among units provided chemoprophylaxis. Several other factors might have contributed to overall reduction in malaria cases in ROK Army such as wearing permethrin-treated military uniform during malaria transmission season and effort made by ROK Government to improve malaria situation in North Korea. However, these measures were not strictly carried out and although the effect of these measures cannot be ignored, we can say that our results represent mostly the effect of chemoprophylaxis. Currently not being done, extensive supervision and surveillance is warranted to ensure that endemic strains of P. vivax in Korea do not become tolerant/resistant to current regimens of chloroquine and primaquine therapy.



 XML Download
XML Download