

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Choriocarcinoma is one of the malignant tumors arising from trophoblastic cells characterized by the secretion of human chorionic gonadotrophin (hCG). The tumor consisted of two basic cell types: cytotrophoblast and hCG-positive syncytiotrophoblast, the typical histologic features of choriocarcinoma (1-5). The serum hCG level is typically elevated, with resultant isosexual pseudoprecocity in children, and menstrual abnormalities, breast enlargement, androgenic changes, or combinations thereof, in adults (1, 2). It usually arises from fetal trophoblasts and rarely arises from germ cells in the testis or ovary or derives from dedifferentiation of other carcinomas (2, 3). The most common sites of systemic metastatic disease are lungs, liver and brain via hematogenous spread (1). Skin is a rare site for metastatic choriocarcinoma, and even more rare as the initial presenting site for the disease (3-5). To the best of our knowledge, about 10 cases of cutaneous metastatic choriocarcinoma were reported in the literature.
We describe a case of 52-yr-old Korean female patient with cutaneous metastasis of choriocarcinoma, diagnosed from a skin biopsy that provided important diagnostic clues to the primary lesion.
CASE REPORT
A 52-yr-old Korean female presented with dyspnea of 2 months duration and cutaneous nodules of 1 month duration on the left side of the neck and the right side of the upper back. Both lesions were fingernail sized rubbery-hard, rapidly growing erythematous nodules. Subjective symptoms such as pruritus or tenderness were not present (Fig. 1). On physical examination, breathing sound was decreased. She had vaginal spotting for 10 days, 1 month prior to her visit. Her past medical history was significant for Behçet's disease, which had been treated with colchicine for the past 4 yr.
Routine blood tests showed leukocytosis with a WBC of 17,780/µL, anemia with a hemoglobin of 9.4 g/dL and slightly elevated hepatic enzyme levels of GOT/GPT at 45/51 IU/L. Chest radiography, chest and abdomen-pelvis CT revealed pleural effusion, innumerable variable sized pulmonary metastatic nodules on both lungs and multiple metastatic lesions on the liver, left adrenal gland and left kidney.
A skin biopsy was performed on the nodule at the right side of upper back. At low magnification, there were several hemorrhagic foci and multiple cellular infiltrations throughout the dermis (Fig. 2A). At high magnification, the infiltrated tumor cells consisted of two cell types, and a biphasic pattern, in close proximity. One element had polygonal shaped, clear cytoplasm and large, irregular shaped, vesicular nuclei with prominent nucleoli, which were identified as cytotrophoblasts. The other cell population showed eosinophilic cytoplasm with cytoplasmic vacuoles and many dark nuclei, which were identified as syncytiotrophoblasts (Fig. 2B). The immunohistochemical staining for hCG antigen (1:600, Polyclonal rabbit, Dakocytomation, Denmark) in the cytoplasm of syncytiotrophoblasts (Fig. 2B inset) was strongly positive, confirming the diagnosis of metastatic choriocarcinoma.
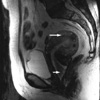
Magnetic resonance (MR) images of the abdomen-pelvis detected diffuse enlargement of the uterus body and a protruding mass in the uterine cavity, which was the primary origin of the tumor (Fig. 3). Her serum hCG level was 700,000 mIU/mL (upper normal limit: 10 mIU/mL). The patient was diagnosed as having a stage IVc disease.
She was referred to the gynecological oncology department, where combination chemotherapy was commenced. During combination chemotherapy, the serum hCG level has fallen off under 2.0 mIU/mL and her skin lesions have almost disappeared. However, 3 months after 17 cycles, total abdominal hysterectomy and bilateral salpingo-oophorectomy were performed due to elevated serum hCG level (4,447.7 mIU/mL), and she is scheduled to receive post-operative adjuvant chemotherapy.
DISCUSSION
Compared to other organs, skin is an uncommon site of metastatic cancer in the body as it is usually associated with a disseminated disease and grave outcome. Occasionally, however, as in our case, cutaneous metastasis may be the first harbinger of a visceral malignancy of unknown origin and gives an important diagnostic clue (3, 4, 6-8).
Cutaneous metastasis of a visceral malignancy has been estimated to be in the wide range of 1.4% to 10.4% according to the type of study undertaken and the site of primary tumor studied (6-11). Involvement of the skin is likely to be near the area of the primary tumor and in proportion to the incidence of internal malignancy. The chest, abdomen, and scalp are common anatomic sites to which metastasis localize with the back and extremities being relatively uncommon areas. Breast cancer in women and lung cancer in men are the most common causes of chest metastatic lesion (6-8).
Occasionally, a cutaneous metastatic lesion may show typical histologic features which give a decisive diagnostic clue to the primary origin. Such cases include mucin-containing cells in colon cancer, bile-containing glandular structure in hepatoma, clear cells in renal cell carcinoma and, like our case, cytotrophoblasts and syncytiotrophoblasts in choriocarcinoma (6).
Choriocarcinoma, in women, is often preceded by a gravid state, which is most often hydatidiform mole (50%), less frequently abortion (25%), and normal term pregnancy (15%). Rarely, it is derived from germ cells in the ovary. In men, it commonly arises from germ cells in the testis (1-5).
The gross appearance of choriocarcinoma is often dark red or purple colored and resembles that of a friable segment of placenta (1). Microscopically, it is characterized by multiple foci of hemorrhage and necrosis around the neoplastic cells, by large sheets of cytotrophoblastic and syncytiotrophoblastic cells, biphasic pattern, and by the absence of hydropic villi. Two populations of the infiltrated tumor cells are mixed in close proximity. The cytotrophoblasts have cuboidal shaped, pale cytoplasm and large, irregular shaped, vesicular nuclei with prominent nucleoli. The syncytiotrophoblasts show eosinophilic cytoplasm with cytoplasmic vacuoles, many hyperchromatic and pleomorphic nuclei with indistinct border, looking like multinucleated giant cells, and may form syncytial knots. The immunohistochemical staining for hCG antigen is positive in the cytoplasm of syncytiotrophoblasts but not in cytotrophoblasts (1-5). Other germ cell tumors such as polyembryoma, embryonal carcinoma, dysgerminoma and mixed germ cell tumor can also show hCG positive syncytiotrophoblastic cells but these tumors do not demonstrate a biphasic pattern consisting of cytotrophoblasts and syncytiotrophoblasts, as in choriocarcinoma (1).
Choriocarcinoma is notorious for its tendency of hematogenous spreading. The most common metastatic sites are, in a descending order of frequency, lung (60-95%), vagina (40-50%), vulva (10-15%), brain, liver (10%), kidney and spleen (<5%). Although choriocarcinomas respond relatively well to chemotherapy, cutaneous metastasis is an extremely uncommon presentation and a poor prognostic sign as it is associated only with disseminated disease (1-5). Chhieng et al. reported a case of cutaneous metastatic testicular choriocarcinoma where the patient died 10 days after the initiation of chemotherapy (4). Shimizu et al. also reported a case of metastatic disease to the upper back of testicular choriocarcinoma, where the patient died 3 months after the appearance of a cutaneous metastatic lesion. In their literature review, of 7 patients with metastatic choriocarcinoma to the skin, 5 patients died within 3 months after the appearance of skin metastasis (3). Chama et al. reported another case of choriocarcinoma with metastasis to the chest wall, which responded well to 12 cycles of combination chemotherapy (5). Our case also responded well to combination chemotherapy. Her cutaneous lesions and symptoms almost disappeared with a striking decrease of serum hCG.
We described an extremely rare patient with metastatic choriocarcinoma presenting initially as a cutaneous lesion. The diagnosis was made from the typical histological findings of a cutaneous metastatic lesion, which was confirmed by immunohistochemical staining for hCG and from the abdomen pelvis MR images. This case highlights the importance of a histological examination of skin metastatic lesion, which can provide conclusive evidences to the diagnosis.


 XML Download
XML Download