

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intrathoracic segment of the subclavian artery is a rare location for a peripheral arterial aneurysm (1-3). Intrathoracic segmental aneurysm is secondary to atherosclerosis, medial degeneration, trauma, and infection. Subclavian artery aneurysms are at an increased risk of rupture, embolization, or thrombosis. Hence, they should be considered for surgical repair. We describe a case of a patient presenting with hoarseness and an expanding intrathoracic mass that was due to a right subclavian aneurysm.
CASE REPORT
A 65-yr-old female presented with hoarseness that began 3 weeks ago. She had no previous history of trauma, pulmonary and bronchial tuberculosis. On admission, her vital signs were normal and blood pressure was equal on both arms. The laboratory workup showed a white blood cell count of 6,500/µL, normal erythrocyte sedimentation rate and C-reactive protein. Syphilis serology, rheumatoid factor, and antinuclear antibody tests were negative. Chest radiograph (CXR) demonstrated a superior mediastinal mass (Fig. 1). Because laryngoscopy showed a fixed right vocal cord, hoarseness was considered to be due to recurrent laryngeal nerve palsy. Computed tomography (CT) and magnetic resonance imaging (MRI) demonstrated a 7 cm sized proximal right subclavian artery aneurysm (Fig. 2, 3). Thoracic and subclavian aortography revealed a tortuous right subclavian arterial anatomy with a saccular aneurysm beginning near the subclavian origin (Fig. 4). The preoperative diagnosis was atherosclerotic right subclavian artery aneurysm.
Repair of the aneurysm was performed through a median sternotomy. We dissected at the aneurysmal afferent loop and efferent loop. We made end-to-end anastomosis by Gore Tex (6 mm sized) graft interposition. In the operation field, we could not find the recurrent laryngeal nerve due to severe adhesions. After the debridement, a partially undetached aneurysm was left.
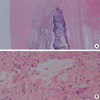
Cultures from the wall of the aneurysm and thrombus were negative. Pathology was consistent with an atherosclerotic aneurysm filled with thrombus (Fig. 5).
After one month follow-up, she still complains of hoarseness and laryngoscopic examination revealed right vocal cord palsy.
DISCUSSION
Aneurysms of the subclavian artery represent about 1% of all peripheral arterial aneurysms (4, 5). They fall into two distinct groups in terms of etiology, presentation, and treatment: those of the intrathoracic and those of the extrathoracic portion of the subclavian artery. Although aneurysms of extrathoracic subclavian artery are related to thoracic outlet syndrome or to previous trauma, intrathoracic segmental involvement is mainly due to atherosclerosis (6).
Intrathoracic aneurysms are most often asymptomatic but can present with symptoms caused by compression or acute aneurysm expansion such as upper chest or shoulder pain, Horner's syndrome, venous congestion, and hoarseness. Symptoms due to distal embolization to the arm are unusual. Extrathoracic aneurysm most commonly presents with a pulsatile mass in the superior fossa and is often tender, which may be noted by the patient or examiner. Brachial plexopathy is another complication of the extrathoracic aneurysm and Horner' syndrome is not infrequent (5-7).
Because isolated true aneurysm of the subclavian artery is rare, the natural history of subclavian artery aneurysm is unclear. It has been reported that an aneurysm of the aberrant right subclavian artery grew at the rate of 0.42 cm/yr measured by CXR (8). In another report, growth rate was reported at 1.31 cm/yr in a true left subclavian artery aneurysm measured by CT scan (9).
Elective surgical repair is the treatment of choice for most subclavian aneurysms, because they have an increased risk of rupture, embolization, thrombosis, and other complications. Intrathoracic subclavian artery aneurysms on the right are best approached by median sternotomy, whereas a high lateral thoracotomy is preferred for the left sided aneurysm (6, 10). Resection or aneurysmorrhaphy is preferred to simple ligation because continued growth and rupture of ligated aneurysm have been reported (11). Recently, as less invasive alternative to surgical repair, endovascular stent-graft treatment is possible (12-15).
We describe a case of a patient who complained of hoarseness and right shoulder pain due to an aneurysm of the intrathoracic subclavian artery. We treated her with graft interposition and left the aneurysm tissue unattached because of severe adhesion.




 XML Download
XML Download