

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Even though esophageal cancer is a common malignancy of elderly patients in Korea, treatment results for these patients are not satisfactory. Patients with metastatic or recurrent esophageal cancer have a particularly poor prognosis owing to their overall medical condition. Palliative surgery to relieve dysphagia results in high morbidity (1). Endoscopic balloon dilation/stent insertion or intraluminal radiotherapy also help to relieve dysphagia with less morbidity than surgery, but the median duration of survival after these treatments is only 3-6 months, which is comparable to that of patients with untreated advanced esophageal cancer (2, 3). For these reasons, chemotherapy has become the primary modality for treating metastatic or unresectable recurrent esophageal cancer, both to relieve symptoms and to prolong life, where possible.
Combination chemotherapy with 5-fluorouracil (5-FU) and cisplatin has been widely used in esophageal cancer, with reported response rates of 35-40% (4). Pre-operative treatment with this regimen was tolerated reasonably well in randomized trials (5, 6), but the median duration of response was generally short, the median survival was only 6-10 months, and efficacy was limited in metastatic disease (7). Paclitaxel, an agent with broad antitumor activity, is one of the most active agents against esophageal cancer, showing response rates in the 30 to 40% when used alone (8) and of 38-48% in combination therapy with cisplatin (9, 10). Given that esophageal cancers respond poorly to other regimens, it is worthwhile to examine the responses of previously treated metastatic or recurrent esophageal cancers to paclitaxel/cisplatin combination chemotherapy. In this study, we evaluated the efficacy and tolerability of biweekly paclitaxel and cisplatin for these patients.
MATERIALS AND METHODS
Patients
Patients with metastatic or unresectable esophageal cancer recurring after previous treatments (chemotherapy, radiation therapy, or surgery) were eligible to participate in this study. The clinical stage of each cancer was evaluated using a complete medical history, physical examination, complete blood count, clinical chemistry, chest radiography, computed tomography of the chest and upper abdomen, and gastrofiberscopy with biopsy. A whole-body bone scan was also performed for cases showing any symptoms suggestive of bony involvement, including abnormalities in serum calcium or alkaline phosphatase levels. Clinical stages for all patients were based on the revised American Joint Committee (AJC) system. Further eligibility requirements were as follows: voluntary informed consent in writing; age <75 yr; Eastern Cooperative Oncology Group (ECOG) performance status ≤2; life expectancy >12 weeks; and adequate hematological, renal, and hepatic function (WBC ≥3,000/µL, granulocytes ≥1,500/µL, platelets ≥100,000/µL, total bilirubin <1.3 mg/dL, and creatinine clearance >60 mL/min). Exclusion criteria were: pre-existing neurotoxicity >WHO criteria grade 1, active infection, other serious underlying medical conditions that would impair the ability of the patient to receive the planned treatment, or inadequate calorie and fluid intake.
Treatment protocol and dose modification
Paclitaxel (90 mg/m2) and cisplatin (50 mg/m2) were administrated by intravenous (i.v.) infusion every 2 weeks. Thirty minutes prior to the paclitaxel infusion, each patient received 20 mg dexamethasone, 50 mg ranitidine, and 5 mg chlorpheniramine maleate i.v., to prevent hypersensitivity reactions. After prehydration with at least 1 L of normal saline, the calculated dose of paclitaxel, diluted in 500 mL of normal saline, was infused over 3 hr. The calculated dose of cisplatin was then administered over 3 hr, followed by posthydration with 3 L of normal saline over 24 hr. Ondansetron (8 mg, i.v.) was routinely given. Patients received further cycles of chemotherapy only when the absolute neutrophil count was ≥1,000/µL and platelets ≥150,000/µL. The paclitaxel dose was reduced to 75% of the original dose in subsequent courses if one of the followings occurred: grade 3 neutropenia with infection; grade 4 neutropenia; grade 3 thrombocytopenia with bleeding that required platelet transfusion; and over grade 3 sensory neurotoxicity. In cases of fatigue or asthenia above grade 3, treatment was postponed for 1 week and restarted when the patient had recovered to below grade 2. After three courses of chemotherapy, progressive patients were excluded. Patients showing disease regression received additional courses of chemotherapy, up to a maximum of eight courses.
Treatment assessment
The clinical restaging procedure included all the studies that had shown abnormal findings prior to treatment. To evaluate toxicity, a physical examination, complete blood count, and blood chemistry were performed at the 8th to 12th day after chemotherapy. To evaluate responses, CT scans of the chest and abdomen, with ultrasonography and endoscopy when appropriate, were repeated after the third and sixth cycles and after the discontinuation of therapy. Responses were evaluated using WHO criteria. A complete response was defined as the complete disappearance of all clinical evidence of disease, persisting for more than 4 weeks. A partial response was defined as a decrease by at least 50% reduction in the sum of the products of the largest perpendicular diameters in all measurable lesions, including esophageal wall thickness or at least a 30% reduction of the largest diameters in uni-dimensional disease (evaluable disease) for at least 4 weeks, with no evidence of progression or of the development of new lesions. Progressive disease was defined as an increase in a previous lesion by more than 25%, or the development of any new lesion. Stable disease was defined as any change in the previous lesion that did not fit into either the partial response or progressive disease categories. DeMeester symptom scores (11) were used by patients to rate their swallowing symptoms on a scale of 0-3 at the beginning of chemotherapy and the best relief during chemotherapy. The scoring system is defined as follows; 0=no dysphagia, 1=mild, i.e. with solids, requiring modification of diet to soft foods, 2=moderate, i.e. difficulty with soft foods, predominantly liquid diet, 3=severe, i.e. obstructed, needing medical intervention for dilatation or bolus obstruction. Toxicities were evaluated according to the National Cancer Institute Common Toxicity Criteria (NCI-CTC).
Statistical methods
Overall survival was measured from the date when the treatment began to the date of death, or of the most recent follow-up visit. The duration of response was measured from the date that the response was noted to the date that progression was confirmed, or to the last visit without progression. The time to progression was measured from the date the treatment began to the date of progression, or to the last visit without progression. The statistical analysis was performed using SPSS software (SPSS, Chicago, IL, U.S.A.). All survival data were updated to June 2004. Median survival times and survival curves were estimated using the method of Kaplan and Meier and were compared using a log-rank test. A value of p=0.05 (two-sided) was considered the limit of significance.
RESULTS
Patient characteristics
Between April 1999 and June 2003, 38 eligible patients with esophageal cancer were enrolled. Of these 38 patients, 6 patients were ineligible: 3 patients had follow-up loss after one cycle of chemotherapy, 2 patients were dropped out because of economic condition and one patient had double primary tumor (esophageal and lung cancer). Therefore, 32 patients were eligible for analysis. Patient characteristics are presented in Table 1. All the patients were male and had confirmed squamous cell carcinoma. Their median age was 60 yr (range 48-74 yr). As indicated in Table 1, 28 patients (88%) had been treated previously. Ten patients (31%) had received neither chemotherapy nor radiotherapy; either metastatic disease was found at diagnosis or they had relapsed after receiving only surgery. Nineteen patients (59%) had received chemotherapy with 5-FU and cisplatin, 18 patients (56%) had received radiation therapy with or without concurrent chemotherapy. Twenty patients (63%) had metastatic lesions. The predominant metastatic sites were the lung, liver, bone, and lymph nodes. All patients evaluated for this study received at least two cycles of chemotherapy.
Chemotherapy delivery
The median number of cycles received was five, with a range of from two to eight cycles; 151 treatment cycles were delivered in total. Of the 32 patients, 26 pateints (81%) received more than three cycles of chemotherapy, and 13 patients (41%) received more than six cycles. No patients had any further treatment after this combination chemotherapy. The median interval between cycles was 19 days (range, 13-36 days), owing to delayed hematologic recovery and asthenia. The planned and achieved dose intensities for cisplatin were 25 mg/m2/week and 19.2 mg/m2/week, respectively; for paclitaxel, they were 45 mg/m2/week and 33.5 mg/m2/week, respectively.
Efficacy
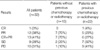
Among the 32 patients, 28 patients had measurable disease and 4 patients had evaluable disease. One patient (3%) showed a complete response (CR), 12 (38%) had partial responses (PR), 9 (28%) had stable disease (SD), and in 10 patients (31%) the disease progressed (PD) (Table 2). The objective response was 41%. The CR patient still had stable disease after three cycles of chemotherapy, but reached CR after six cycles. Seven partial responses were seen among the 10 chemotherapy-or radiotherapy-naive patients, and 6 of 22 patients previously treated with chemotherapy or radiotherapy responded either completely (one patient) or partially (five patients). The objective response among naive patients was significantly higher than among the others (p=0.049, two-sided Fisher's exact test). Follow-up dysphagia scores were available for 29 patients. 11 patients (34%) had an improvement of at least one grade in dysphagia score after treatment and 12 patients (37%) showed no change of swallowing difficulty. Only 6 patients (19%) had a progression of dysphagia. For responders, the median duration of response was 4.5 months (range, 1.0-49.2 months), and the median time to progression for all patients was 5.0 months (range, 1.3-52.6 months).
Safety
The main hematologic toxicities observed were anemia and neutropenia. Over grade 3 of neutropenia and anemia were observed in 6 (19%) and 5 (16%) patients, respectively. Thrombocytopenia was rare. Neutropenic infection developed in 2 patients (6%) with pneumonia, who recovered after treatment with antibiotics. Grade 1 or 2 sensory neurotoxicity was observed in 10 patients (50%); sensory neurotoxicity over grades 3 did not occur. The major non-hematologic toxicity was fatigue, which spontaneously resolved after 1 or 2 weeks of rest. One patient developed grade 3 hepatotoxicity after six cycles of chemotherapy. Therapy was stopped, and the patient recovered spontaneously after 2 months. There was no treatment-related mortality. There were no significant differences in hematologic or non-hematologic toxicities between chemotherapy-or radiotherapy-naive patients and the others (Fig. 1).
Survival
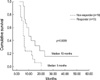
The median overall survival time of all patients was 7 months (95% CI, 5.13-8.87). The median overall survival time of responding patients was 10 months (95% CI, 4.95-15.05; range, 5-51 months) compared with 5 months (95% CI 3.85-6.15, range 2-20 months) for non-responding patients. This increased survival time was significant (p=0.0069). The 1-yr and 2-yr survival rates of all patients were 28.1% and 7.1%, respectively (Fig. 2).
DISCUSSION
Esophageal cancer is one of the most difficult malignancies to manage, with early extension into adventitia or through the esophageal wall, and regional lymph node involvement by the time of diagnosis. Despite treatment with aggressive surgical resection, the overall 5-yr survival rate is only 20%, and the majority of patients relapse both locoregionally as well as at distant sites (12, 13). To overcome this poor prognosis, multimodal treatment is playing an increasingly important role in the management of esophageal cancer. Currently available preoperative chemoradiation therapy, followed by surgery, achieves a complete response in 20-40% of patients, with a 5-yr survival of 25-35% (14, 15). However, half of all patients are unresectable or metastatic at presentation, and 65-75% relapse after surgical resection. The effect of chemotherapy on survival in patients with metastasis or relapsed disease is unclear, owing to a lack of randomized phase III trials comparing chemotherapy to best supportive care. Nevertheless, chemotherapy would be warranted if it led to palliation of symptoms and/or to prolongation of life.
Reduced tolerance to toxic chemotherapy regimens in patients with metastatic or recurrent esophageal cancer is the result of larger tumor burdens, older ages, and comorbidities attributable to tobacco use and alcohol consumption. Hence, different chemotherapy regimens are needed for these patients. Bleiberg et al. (7) reported a response rate of 35% in metastatic esophageal cancer to combination chemotherapy with 5-fluorouracil and cisplatin. In spite of this response rate, this regimen is not the standard treatment for metastatic esophageal cancer, owing to a high incidence of treatment-related deaths (16%).
Recently, several new agents such as paclitaxel, irinotecan, and vinorelbine have shown promising activity in the treatment of refractory or metastatic esophageal cancer (8, 16, 17). Petrasch et al. (18) treated 24 patients with cisplatin (50 mg/m2) and paclitaxel (90 mg/m2), administered biweekly. Patients in that study had metastatic or relapsed disease after surgery, without previous chemotherapy. They had a response rate of 40%, and a median of 8 months progression-free survival. Even though the response rates of Petrasch's and our report were similar, the progression-free survival is different (8 months vs. 5 month, respectively). It may be originated from the low achieved dose intensity in this study. Van der Gaast et al. (19) used higher doses (60 mg/m2 cisplatin, 180 mg/m2 paclitaxel). Using the same high doses, Polee et al. (20) reported a 43% response rate, but 31% of patients showed grade 3 or 4 neutropenia, and 63% had grade 1 or 2 sensory neurotoxicity.
In this study, 28 patients (88%) had been treated previously, 22 (69%) of those with chemotherapy or radiotherapy. The overall response rate was 41%, comparable to that seen by Polee et al. with higher doses of paclitaxel and cisplatin. The objective response was higher in chemoradiotherapy-naïve patients (70%) than in others (27%), and this combination chemotherapy dose may be satisfactory for these patients. Responders to chemotherapy also had a significant survival benefit compared with non-responders, showing the effectiveness of chemotherapy for metastatic or recurrent esophageal cancer.
Although squamous cell carcinomas have become increasingly less common over the past two decades and now account for approximately 40% of all esophageal malignances reported, all of our patients had confirmed squamous cell carcinoma and this result showed the high activity of combination therapy for tumors of this histology (21, 22). Considering the poor medical condition usually associated with previously treated patients, this regimen was fairly well tolerated. Although 6 patients (19%) developed grade 3 or 4 neutropenia, serious infections were not observed. Sensory neurotoxicity was seen in 16 patients (50%), all with grade 1 or 2. It seems to be associated with dose reduction as toxicity grading, and there was no severe sensory neurotoxicity including motor weakness. No significant differences were noted in hematologic or non-hematologic toxicities between chemoradiotherapy-naïve patients and the others.
At the point of the aim of palliative therapy, the improvement of dysphagia via tumor regression is important. In this study, 11 patients (34%) showed the improvement of dysphagia. 12 patients (37%) had no change of dysphagia, but 5 patients of them showed no dysphagia (score 0) at the beginning of treatment and maintained normal swallowing during treatment. Remainder of them also maintained as a state of solid intake (score 1).
In conclusion, a biweekly schedule of paclitaxel and cisplatin at the dose used in this study is not only effective and well tolerated in metastatic or recurrent esophageal cancer patients, especially in chemotherapy- or radiotherapy-naive patients, but also effective in improvement of dysphagia. Although moderate effects were shown in patients that had been treated previously with chemotherapy or radiotherapy, further study of other, perhaps higher, doses of paclitaxel or cisplatin may be needed to improve responses in these patients.


 XML Download
XML Download