

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Multiple myeloma (MM) is a malignant plasma cell disorder accounting for ~10% of hematological malignancies that frequently involves old age patients. The incidence of multiple myeloma has been increasing since the 1980s in Korea (1). Treatment options for patients with symptomatic MM range from relatively simple conventional chemotherapy to high-dose chemotherapy followed by peripheral stem cell or bone marrow transplantation (2).
For the last several decades, conventional chemotherapy using melphalan and prednisolone was the mainstay of myeloma treatment that produced response rates of 50-60%. But, complete remission (CR) was less than 5%, and median remission duration and overall survival (OS) were 18 and 30-36 months (3, 4). There is no evidence that additional cytotoxic agents, such as doxorubicin and nitrosourea, offer survival advantages compared with that achieved with melphalan and prednisolone (5). High-dose chemotherapy followed by hematopoietic stem cell transplantation has been shown to increase the percentage of CR to almost 50% in selected patients. Although conventional chemotherapy and high-dose therapy with hematopoietic stem cell rescue can prolong survival, few, if any, patients are cured (6-10). However, salvage therapies for these patients with relapsed or refractory MM are disappointing, and although thalidomide has shown some promise (11-15), more effective treatment strategies are urgently required.
Recent clinical trials showed that bortezomib (Velcade®, formerly PS341), a novel proteasome inhibitor, had therapeutic activity in patients with relapsed or refractory myeloma (16, 17). Richardson et al. reported that the response rate to bortezomib was 35% and a median duration of response was 12 months in relapsed or refractory myeloma (16). However, only 2 phase II clinical trials that showed the efficacy of bortezomib in myeloma patients were published (16, 17) and no data is available upon bortezomib in Korean patients with relapsed or refractory MM. Therefore, a pilot study of bortezomib in these myeloma patients was conducted in 3 institutions. This pilot study aimed to assess the feasibility of bortezomib in Korean patients.
PATIENTS AND METHODS
Patients
The eligibility criteria for patients were as follows; 1) patient age ≥18 yr, 2) multiple myeloma which was relapsed or refractory to previous chemotherapy or autologous stem cell transplantation, 3) patients with measurable disease [M-protein], 4) an ECOG performance status of 0-3, 5) aspartate aminotransferase or alanine aminotransferase ≤3× upper limit of normal, and total bilirubin ≤2× upper limit of normal, 6) creatinine clearance ≥10 mL/min, 7) platelet count ≥30×109/L, hemoglobin ≥8.0 g/dL and absolute neutrophil count ≥0.5×109/L. All patients gave written informed consent before study entry.
Treatment
Patients received bortezomib (Velcade®, 1.3 mg per square meter of body-surface area) as an intravenous bolus (taking 3 to 5 sec to administer) twice weekly for 2 weeks (days 1, 4, 8 and 11) in a 21-day cycle. Treatment was withheld from patients with drug-related grade 3 or worse non-hematologic adverse events or grade 4 hematologic adverse events until the events had diminished to grade 1 or better. Then, treatment was resumed at a dose of 1.0 mg per square meter upon resolution of the adverse events. Further reduction to 0.7 mg per square meter was allowed, but lower doses were not permitted. Patients with no change or progressive disease after 2 cycles were permitted to receive 20 mg of oral or intravenous dexamethasone on the day of and the day following each dose of bortezomib.
Assessment of efficacy and safety
The primary end-point was overall response rate to bortezomib. Response to bortezomib was evaluated according to the criteria of the European Group for Blood and Marrow Transplantation (EBMT) (18) before initiation of each bortezomib chemotherapy cycle. Complete remission (CR) was defined as the absence of M-protein on immunofixation (or immunoelectrophoresis) for 6 weeks and 5% or fewer plasma cells in the bone marrow, with no increase in size or number of bone lesions and the disappearance of soft tissue plasmacytomas. Partial remission (PR) was defined as ≥50% decrease of serum M-protein and/or ≥90% decrease of urine M-protein for 6 weeks, with no increase in size or number of bone lesions. Minimal response (MR) was defined as 25-49% decrease of serum M-protein and/or 50-89% reduction in urine M-protein, which still exceeded 200 mg/day for 6 weeks. No change (NC) was defined as not meeting the criteria of either minimal response or progressive disease, and progressive disease (PD) was defined as ≥25% increase of serum M-protein, which must have represented an absolute increase of at least 0.5 g/dL, and/or ≥25% increase of urine M-protein, which must have represented an absolute increase of at least 200 mg/day and have been confirmed by at least one repeated test.
Adverse events were graded according to the National Cancer Institute Common Toxicity Criteria, version 2.0, from the first dose until 20 days after the last dose of bortezomib.
Statistical analysis
Time to progression (TTP) was defined as the interval from the initial administration of bortezomib to disease progression. Overall survival (OS) was defined as the time elapsed from the onset of bortezomib to death whatever the cause of death. Distributions over time were estimated by Kaplan-Meier analysis.
RESULTS
Patient characteristics
Seven patients were accrued onto this study between November 2003 and April 2004 from 3 centers. All 7 patients had measurable serum M-protein amount. The median age was 59 yr (range: 57-67 yr). All patients previously received VAD (vincristine, doxorubicin and dexamethasone) and thalidomide (±dexamethasone) chemotherapy. Three patients previously received alkylator-containing chemotherapy and 4 patients received autologous peripheral blood stem cell transplantation. Table 1 shows the summary of base-line characteristics and treatment courses of enrolled patients.
Treatment and efficacy
A total of 20 cycles of bortezomib and/or dexamethasone treatment was performed (Table 1). Among 3 patients who experienced NC after 2 cycles of bortezomib treatment, dexamethasone was added to the bortezomib treatment regimen in 2 patients (case 4 and 6) in cycle 3. Two patients (case 3 and 7) received only one cycle of bortezomib; additional bortezomib chemotherapy was not performed in one patient (case 7) because of disease progression and the other (case 3) received tandem autologous stem cell transplantation after achievement of PR following one cycle of bortezomib. Two patients (case 2 and 5) received 2 cycles of bortezomib; one patient (case 2) dropped out of the study because of the economic problem for the treatment and the other patient (case 5) with the response of NC after 2 cycles of bortezomib received other salvage chemotherapy. As shown in Table 1, 3 patients (43%) achieved PR. Three patients (43%) experienced NC and one patient (14%), PD. Among 2 patients who experienced NC after 2 cycles of bortezomib monotherapy and received additional dexamethasone in cycle 3, 1 patient (case 6) achieved PR after the addition of dexamethasone. So, overall response to bortezomib and/or dexamethasone was 57%.
Adverse events
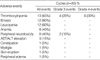
Commonly reported adverse events in this pilot study are shown in Table 2. Thrombocytopenia, emesis, leucopenia, anemia, peripheral neuropathy and hepatic enzyme elevation were common. Emesis was mild to moderate and easily manageable with routine support. The most commonly reported serious adverse event was thrombocytopenia (grade 3/4, 10 of 20 cycles (50%) and 4 of 7 patients (57%)). Grade 3 peripheral neuropathy developed in 2 of 20 cycles (10%) and 1 of 7 patients (14%). There was no treatment related mortality.
Drug-related adverse event led to discontinuation of bortezomib therapy in 1 patient (case 6). After 2 cycles of bortezomib monotherapy and 4 cycles of bortezomib/dexamethasone combination, this patient suffered from severe pneumonia and needed mechanical ventilation care. After recovery, peripheral neuropathy (grade 3) persisted and further administration of bortezomib was not done.
Time to progression and overall survival
Median follow-up duration was 10.5 months (range 6.4-11.2 months). During follow-up period, four cases (57%) showed increased M-protein amount (disease progression) during or after the completion of bortezomib and/or dexamethasone treatment. Other two patients received another treatment after documentation of PR (case 3) and NC (case 5). These two patients (case 3 and 5) were considered as 'censored' cases in this study. Only one case (case 2) was in the status of continuous PR at the last follow-up. When time to progression (TTP) was defined as the interval from the initial administration of bortezomib to disease progression, median TTP in patients who received bortezomib and/or dexamethasone was 5.1 months (95% confidence interval: 3.3-6.9 months). During the follow-up period, four patients (57%) were still alive and three patients died. Cause of death was disease progression in all three patients (Table 1).
DISCUSSION
The proteasome is a multi-enzyme complex that is present in all cells. It degrades proteins that regulate cell-cycle progression (19, 20) and causes proteolysis of IκB the endogenous inhibitor of nuclear factor-κB (NF-κB). Degradation of IκB by proteasome activates NF-κB, which up-regulates the transcription of proteins that promote cell survival, stimulate growth, and reduce susceptibility to apoptosis. Also, NF-κB activation induces drug resistance in myeloma cells (16). Bortezomib, a boronic acid dipeptide, reversibly inhibits proteasome function by targeting the chymotrypsin-like site of the proteasome (21) and has antitumor activity in a variety of in vitro and in vivo models of tumors. It induces apoptosis in myeloma-cell lines (22, 23). Molecular mechanisms of bortezomib entail more than NF-κB inhibition (24, 25), and in vivo, it enhances the anti-myeloma activity of chemotherapeutic agents (24, 26).
Based on a phase I study of advanced hematologic cancer, in which bortezomib showed activity in 9 patients with MM (27), 2 phase II trials in relapsed or refractory myeloma were reported until now (16, 17, 28). In these 2 studies, overall response rate to bortezomib alone was 33-50% (16, 17). The median duration of response in responders was 12.0 months and median time to progression among all enrolled patients was 7.0 months (16). The overall response rate of bortezomib and/or dexamethasone was 44-62% (17).
In this pilot study, overall response rate to bortezomib alone was 43%, which was similar to previous reports, and 1 additional PR was achieved with the combination of bortezomib and dexamethasone (case 6). Considering that all enrolled patients previously received chemotherapy (±autologous stem cell transplantation) and thalidomide, bortezomib seems to be effective in chemotherapy and thalidomide-failed myeloma patients. As previous reports, serious thrombocytopenia and peripheral neuropathy were developed. The incidence of grade 3 and 4 thrombocytopenia was 50% in this study. This more frequent incidence of serious thrombocytopenia than previous reports (16, 17) might be caused by patient characteristics of this study, in which all of enrolled patients received bortezomib as 3rd to 6th-line treatment and seemed to have poor bone marrow functions. Median TTP in this study, when bortezomib and/or dexamethasone were administered, was 5.1 months. These toxicity profiles and survival data need to be determined in future larger studies on Korean patients.
Overall, bortezomib seems to be effective and feasible in chemotherapy and thalidomide-failed myeloma patients with the dosage of 1.3 mg per square meter twice weekly for 2 week in a 3-week cycle. These observations necessitate the conduction of future larger clinical studies on Korean patients to characterize clinical efficacy and safety of bortezomib more precisely.

 XML Download
XML Download