

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
It is known that fatigue and chronic fatigue (CF) are common in patients visiting primary care institutions. Since the concept of chronic fatigue syndrome (CFS) emerged in Western countries in the 1980s, there have been many epidemiological and clinical researches on CF and CFS. The term and definition of CFS were first suggested by the Centers for Disease Control and Prevention (CDC) of the U.S.A. in 1988 and new diagnostic criteria were established by CDC in 1994, which have been widely accepted until now (1, 2). The pathophysiologic mechanism of CFS is not clear yet. However, multiple somatic and psychological symptoms as well as CF significantly disabling everyday life are distinct in patients with CFS.
According to Western researches, CF disabling everyday life for over six months is found in 5-15% of patients visiting primary care institutions and 1-10% of general population; and the prevalence of CFS is as low as 0.5-2.5% of patients visiting primary care institutions and 0.2-0.7% of general population (3-6). In a recent study in Korea on 1,000 patients who visited the primary care center of a university hospital, the prevalence of CF was 11.4% and that of CFS 1.22% (7).
However, there have been only a few epidemiological studies on CF and CFS in Korea and no such study has been performed in general population or in those visiting primary care institutions in local communities. Thus we conducted this study to estimate the prevalence of CF and CFS in patients visiting community-based primary care clinics in Korea. We also investigated the sociodemographic and clinical characteristics of CF and CFS.
MATERIALS AND METHODS
Subjects
The study subjects were 18 yr old or older patients who visited one of eight community-based primary care clinics in Korea. This study was done between the 7th and 17th of May 2001. Among the eight community-based primary care clinics (all were Family Medicine), 5 were in Seoul, the metropolitan area, 1 in Gangwon-do, 1 in Chungcheong-do, and 1 in Jeju-do. Patients who refused to participate in the study or did not answer the questionnaires appropriately were excluded, but there were no other specific exclusion criteria. During the study period, a total of 1,962 patients attended to eight primary care clinics and 1,648 of them participated in this study.
Questionnaires
All the participants were given self-reporting questionnaires, and those who had difficulties in completing the questionnaire were interviewed by trained nurses. The questionnaire survey was conducted in two stages. In the first stage, the 1,648 participants were questioned on their socio-demographic characteristics and fatigue. Socio-demographic characteristics included age, gender, educational qualification, employment, and marriage as well as habits such as drinking and smoking. In addition, the questionnaire included questions on present and past history of illness and medicines being taken currently. Whether the subject was fatigued or not was determined by the question of 'Have you ever felt fatigue as disabling your everyday life substantially during the last one month?' and those who replied 'Yes' were directed to a question how long the fatigue had lasted. The period of fatigue was divided into '1-6 months' and 'Over 6 months.' In the second stage, another questionnaire was conduced on 139 patients with CF who replied that their fatigue had continued for over 6 months. The questionnaire was composed of questions on the symptoms of CF based on the case definition of CFS and another eight symptoms, questions to screen depression, and questions to measure the intensity of stress. The questions related to CFS included the symptoms of CF and another eight symptoms based on the case definition of CFS proposed by CDC in the U.S. in 1994 (2). Depression was screened by the Zung's self-rating depression scale (8). The intensity of stress was measured using BEPSI-K (9).
Classification of subjects
The 1,648 subjects participating in the study were classified into 'No fatigue,' 'Prolonged fatigue (fatigue for 1-6 months)' and 'CF (fatigue for over 6 months)' according to whether they had fatigue and how long the fatigue had lasted. Because fatigue for more than one month was clinically significant, the patients complained of fatigue for less than one month were classified as 'No fatigue' (10). The physicions evaluated the CF patients through history taking, physical examinations, and laboratory tests, and determined whether the cause of CF could be medically explained or not. Laboratory tests-complete blood count with differential, blood chemistry (liver function test, electrolytes, and lipid profiles), thyroid function test, urinalysis, chest radiography, etc.-were selected with reference to the tests for CF patients recommended by CDC in 1994 (2). In addition, additional tests were performed as necessary. Through this process, CF patients were further categorized into four sub-groups. They were categorized as 'Explained CF' if the cause of CF could be medically explained, or as 'Unexplained CF' if the cause of CF could not be medically explained. 'Explained CF' was divided into 'Physical CF' and 'Psychological CF' according to the major cause of CF. If there were two or more causes that could explain CF, the most relevant single cause was considered to be the major problem associated with CF by physicians' decision. The subjects with unexplained CF who met the case definition criteria for CFS were classified as CFS and the others of unexplained CF did not meet the criteria were classified as idiopathic chronic fatigue (ICF) (2). The classification of CF patients and diagnosis of CFS (including ICF) were made by each physician after evaluating the CF patients at least three times.
Analysis
The point prevalence and 95% confidence interval (CI) of CF and CFS were calculated by the percentages of patients classified into CF and CFS among the 1,648 participants. Because the 314 patients who did not participate in the study were not statistically different from the 1,634 participants in terms of gender and age, they were excluded from analysis. We also estimated the age-sex adjusted prevalence of CF and CFS based on the Korean population distribution in 2000. We estimated the point prevalence of prolonged fatigue and CF according to the age and sex distribution. Comparative multivariate analysis was done on socio-demographic characteristics among the three groups-no fatigue, prolonged fatigue, and CF. Major causes of explained CF were identified and their frequencies were counted. In addition, the four groups of CF were compared with regard to their socio-demographic characteristics, the intensity of stress, the frequency of depression, etc. The frequencies of the CF symptoms and another eight symptoms included in the case definition of CFS were comparatively analyzed. The level of statistical significance was set at 5%, and SAS 6.12 for Windows was used for analyses.
RESULTS
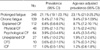
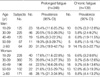
Among the 1,648 subjects, 348 complained of prolonged fatigue, showing a point prevalence of 21.1% (95% CI 19.1-23.1%), and 139 of CF, showing a point prevalence of 8.4% (95% CI 7.1-9.7%). Among the cases of CF, 80.5% were explained CF, of which 42.9% (48 patients) were physical CF and 57.1% (64 patients) were psychological CF. The point prevalence of unexplained CF was 1.6% (95% CI 1.0-2.2%), and those of CFS (10 patients) and ICF (17 patients) were 0.6% (95% CI 0.2-1.0%) and 1.0% (95% CI 0.5-1.5%), respectively. Age-sex adjusted point prevalences of CF and CFS were 9.4% (7.9-1.09%) and 0.7% (0.3-1.2%) (Table 1). The prevalence of CF in men was higher in the age groups over sixty than in the other age groups, and that in women was the highest in the age group fifty to fifty-nine (Table 2).
The percentage of patients complaining of prolonged fatigue or CF was relatively higher with aging (p=0.001) and educated population (p=0.002) compared to that of no fatigue. In addition, compared to those with a spouse, patients who were bereaved of, divorced by, or separated from the spouse tended to complain more of prolonged fatigue or CF (p=0.001) (Table 3).
Among the cases of explained CF, 64 patients (57.1%) had psychosocial causes while 48 patients (42.9%) had physical causes. Stress was found to be the most frequent cause (23 patients, 16.6%), followed by of depression, adjustment disorder, diabetes (uncontrolled), asthma, anxiety neurosis, chronic hepatitis, tuberculosis, etc. (Table 4).
With regard to socio-demographic characteristics and personal habits, the drinking rate was significantly higher in the group of physical CF than in the other three groups (p=0.018), and educational qualification was higher in the group of unexplained CF than in that of explained CF (p=0.038). However, no statistically significant difference was observed in age, gender, occupational characteristics, and marital status among the groups. The frequency of stress was significantly higher in the group of psychological CF than in the other groups (p=0.002), and that of depression was significantly higher in the groups of psychological CF and CFS than in those of physical CF and ICF (p=0.001 in all) (Table 5).
Patients with CFS patients showed high frequencies in all of the eight symptoms included in the diagnostic criteria for CFS as well as in impaired short-term memory or concentration, unrefreshing sleep, multi-joint pain without arthritis, and post-exertional malaise lasting more than 24 hr. In addition, the tenderness of cervical and axillary lymph nodes and muscle pain showed higher frequencies in the CFS than in that of explained CF (physical and psychological CF) (Table 6).
DISCUSSION
This is the first study that investigated the point prevalence of CF and CFS in patients who visited community-based primary care centers in Korea. There have been many epidemiological researches on CF and CFS in Western countries since the 1990s, but such studies have been quite limited in Korea. A recent Korean study focused on patients who visited a primary care center of a university hospital (7). Although our study is not on the prevalence of CF and CFS representing the general population of Korea, we expanded the scope of subjects to patients who visited one of eight community-based primary care clinics in Korea.
According to the results of this study, the prevalence of CF as serious as disabling everyday life for over 6 months was 8.4% (95% CI 7.1-9.7%), which was similar to 5-15% in foreign researches (on patients visiting primary care institutions) but was lower than 11.4% in a study in Korea on patients who visited a university hospital (3-7, 11-14). The difference might be due to different study subjects. In this study, 10 out of 1,648 subjects were found to have CFS, so the point prevalence of CFS was 0.6% (95% CI 0.2-1.0%) and only 7.2% of CF patients had CFS. We speculate that CFS was distinguished from most CF by the uncertainty of its cause and several characteristic symptoms including fatigue. And this point prevalence of CFS was lower than 1.22% reported by a previous study in Korea (on patients visiting a university hospital) (7). In addition, this prevalence was lower than 0.2-2.5% reported by researches in Western countries and the difference is thought to have resulted from racial difference. According to the report of a research on patients at a certain region in the U.S., prevalence of CFS was 1.0% among whites, 2.75% among blacks and 0.12% among Asians (15). And a Japanese study from a nationwide survey reported the prevalence of CFS was 0.85 per 100,000 persons during 1992 (16). As for the difference of CFS prevalence between our study and the Japanese study, it should be noted that the diagnostic criteria of CFS in the Japanese study was based on CDC in 1988 and the study subjects were general population.
Patients with explained CF were 80.5% of CF cases, and psychosocial causes (57.1%) were more frequent than physical causes (42.9%). The most common cause was stress, followed by depression, adjustment disorder, diabetes (uncontrolled), asthma, anxiety disorder, etc. In several researches in Western countries, the major causes of CF were reported to be psychological disorders, and the result of our study is consistent with that of the previous study in Korea (7, 17, 18). Thus, it is considered that stress is the major cause of CF and psychosocial causes are more frequent than physical ones in Korea.
Subjects classified as prolonged fatigue and CF tended to be older, without a spouse, and have higher educational qualification compared to those classified as no fatigue. Although several researchers reported that fatigue has no age predilection, it was reported that fatigue is more common in adults than in children and adolescents and its frequency increases with age from middle age to older ages (19, 20). In addition, it was reported that fatigue is inversely proportional to economic level and the intensity of fatigue is lowest in the highest socio-economic class (21, 22). These results may be due to the different perception of fatigue, which is a subjective symptom, but further epidemiological research is needed in Korea.
We compared CFS with the other three groups of CF in order to identify their socio-demographic and clinical characteristics, but it was difficult to delineate clinical characteristics of CFS because the number of subjects with CFS (10 patients) in our study was too small. In addition, there were no socio-demographic characteristics that showed a significant difference compared to the other three groups. However, among the eight other symptoms of the CFS diagnostic criteria except fatigue, the tenderness of cervical or axillary lymph node (60%), multi-joint pain without arthritis (80%), and muscle pain (90%) showed higher frequencies in the CFS group than in the other three CF groups (although the difference was not significant with the ICF group). Since the eight symptoms are included in the diagnostic criteria for CFS, it seems natural that their frequencies are higher in the group of CFS than in explained CF. And due to the bias of this univariate analysis, it was not conclusive whether these symptoms were distinct in CFS from explained CF. However, these symptoms are known to be related to infection resulting from abnormal immune function, so this result may provide a clue to the opinion that CFS is related to infection or immunity. Several researches have shown that many flu-like symptoms observed in CFS patients are caused by an immune disorder (23, 24).
Previous researches have demonstrated that CFS is frequently accompanied with emotional disorders such as depression and anxiety (25, 26). And according to the result of a meta-analysis on medically unexplained physical symptoms and depression and anxiety, CFS had a higher frequency of depression than irritable bowel syndrome and a higher frequency of anxiety than fibromyalgia (27). In this study as well, 80% of CFS showed depression.
The limitations of this study are as follows: since the subjects of this study were patients visiting community-based primary care clinics, their point prevalence of CF and CFS may not represent those of the general population. And the population distribution of the patients who visited the eight primary clinics participated in this study might not be consistent with the one from the entire community-based primary care in Korea. In addition, because both the previous study in Korea and the present study focused on patients visiting medical care institutions, future studies on the general population in Korea may report a lower prevalence of CF and CFS. The second limitation is the possibility that the decisions made by physicians in the eight community-based primary care clinics to investigate the cause of CF might not have been completely consistent although they analyzed the cause of CF based on objective criteria. The third limitation is related to the number of subjects. In order to estimate the prevalence of a rare disease like CFS, a larger number of subjects are required. If the number of subjects is not big enough, the prevalence may be underestimated or overestimated. Lastly, not all patients during the study period were included in the study. Among the 1,962 patients who visited medical care institutions during the study period, 15% (314 persons) were excluded from the study. If they were included in the analysis, the point prevalence of CF and CFS was likely to be different. However, no statistical difference was found in terms of age and sex between the 314 non-participants and 1,648 participants.
Despite these limitations, this study is meaningful in that it is the first study on patients visiting one of eight community-based primary care in Korea to investigate the point prevalence of CF and CFS. The results of this study are expected to be utilized in future epidemiological research on CF and CFS in the general population in Korea.




 XML Download
XML Download