

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastrointestinal stromal tumors (GISTs) are usually resistant to conventional chemotherapy. So, in case of unresectable or metastatic GIST, the prognosis was poor. However the prognosis of GIST has been changed dramatically after the introduction of imatinib mesylate (Glivec, previously called STI571). Imatinib inhibits not only bcr-abl tyrosine kinase and platelet-derive growth factor (PDGF), but also c-KIT kinase which is constitutively activated in GISTs. By this reason, imatinib becomes to be wide use for the treatment of GIST as well as chronic myeloid leukemia. Imatinib is relatively safe drug comparing with conventional cytotoxic drugs. Its adverse events were reported from several clinical trials. Common adverse events were usually mild and included nausea, edema, cramps, diarrhea, vomiting, rash, headache, fatigue, and arthralgia (1-5). In addition, severe or rare adverse events of imatinib have been reported, including severe skin rash, hair repigmentation, splenic rupture, bone marrow necrosis, and male gynecomastia. We report here a case of male gynecomastia coincident with testicular hydrocele in a patient treated with imatinib for metastatic GIST. Gynecomastia and testicular hydrocele are thought to be induced by imatinib through inhibition of c-KIT and PDGF. We will discuss the possible mechanisms of gynecomastia and testicular hydrocele.
CASE REPORT
A 42-yr-old man visited our hospital for management of liver masses. Two years earlier, he had undergone small bowel resection for removal of a 20 cm-sized mass, later shown to be a GIST. Following resection, he received postoperative adjuvant radiation therapy, at a total dose of 5,040 cGy. Upon presentation, multiple hepatic masses were revealed by computed tomography (CT). A paraffin block specimen of the previously resected small bowel mass was then reviewed. This tumor consisted of polygonal to spindle cells with moderate cellularity. The tumor cells showed pleomorphism, and necrosis was present. The mitotic figures were not frequent (2/50 high power fields). The tumor cells were immunohistochemically positive for c-Kit and focally positive for SMA, but negative for CD34 and S100, supporting the original diagnosis of GIST of interstitial cells of Cajal origin.
He was prescribed oral imatinib mesylate 400 mg daily. Just after starting drug treatment, the patient complained of periorbital swelling, but no dose reduction was required. Three months later, the hepatic lesions improved, showing a partial response, and nine months after his first visit to our hospital, CT scan and positron-emission tomography showed no evidence of disease. Treatment was discontinued after a further 5 months of imatinib mesylate, but a CT scan performed 3 months after finishing imatinib showed disease progression. A second period of imatinib treatment was started, at the same dose of 400 mg/day. One month later, the patient complained of breast pain and scrotal swelling. Physical examination revealed right gynecomastia and right painless scrotal swelling. A precise medical history was taken, at which point it was learned that left painful gynecomastia and scrotal swelling had developed during the first period of imatinib treatment, but that both had improved after stopping imatinib.
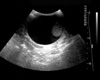
Pain in the right breast began on the 20th day of the second period of imatinib treatment. Decreased libido and impotence were noted. A testicular ultrasonogram showed a large amount of fluid in the right scrotal sac and his right testis was displaced downward (Fig. 1). The left scrotum and testis and the bilateral spermatic cords were normal. The patient was diagnosed with non-communicated testicular hydrocele.
The hormonal status of the patient was evaluated. Thyroid function test was within normal ranges. His serum thyroid stimulating hormone level was 1.1 µU/mL, his free T4 concentration was 1.3 ng/dL, his serum luteinising hormone level was 6.8 IU/L, and his follicle-stimulating hormone level was 14.1 IU/L. His serum testosterone concentration had decreased to 2.3 ng/mL. Androgen support was started and hydrocelectomy was performed. Pathologic examination of the hydrocele specimen showed it to be fibroadipose tissue without lining mesothelium. His gynecomastia improved after androgen support.
DISCUSSION
The most common adverse events of imatinib mesylate include edema, diarrhea, myelosupression, muscle cramps, skin rash, and conjunctival inflammation, most of which are mild (3, 6). In addition, rare or severe adverse events were reported. There have been case reports of severe skin rash, Stevens-Johnson syndrome, and an acute generalized exanthematous pustulosis in patients treated with imatinib (7, 8), and 9 patients (5 men and 4 women) with gray hair before treatment had progressive repigmentation during imatinib treatment (9). In contrast to the repigmentation, imatinib mesylate-induced hypopigmentation was also reported (10-12). Among the more than 10,000 chronic myeloid leukemia (CML) patients treated with imatinib, there have been 3 reported cases of splenic rupture (13), and bone marrow necrosis (14), possibly due to increased apoptosis and the release of prothrombotic cellular material, has been reported. Imatinib was originally developed for inhibition of bcr-abl tyrosine kinase. However it is known that imatinib can also inhibit c-KIT tyrosine kinase and platelet-derived growth factor receptor (PDGFR) tyrosine kinase. The inhibition of c-KIT or PDGF is thought to be responsive for some of these adverse events.
A recent report has described seven cases of gynaecomastia (one grade 1 and six grade 2) in 38 CML patients treated with imatinib (15). PDGF signaling is important in testes organogenesis and Leydig cell differentiation (16). Also, PDGF-A is obligatory for adult Leydig cell recruitment and spermatogenesis (17). c-Kit activity is modulated by stem cell factor which in combination with insulin-like growth factor had effect on leuteinizing hormone receptor and increased the expression of StAR, CYP11A, CYP17, and 3β-hydroxysteroid dehydrogenase mRNA expression (18). Therefore, imatinib can reduce testosterone biosynthesis by inhibiting c-KIT and PDGFR in the testis, and male gynecomastia can result from decreased testosterone (19, 20). In previous report, rise of progesterone and 17-hydroxyprogesterone could represent the accumulation of testosterone precursors as a consequence of impairment of key enzymes in the steroidogenic cascade (15). In our report, decreased testosterone was detected during gynecomastia, and testosterone supply improved gynecomastia and libido.
In our patient, the relationship between imatinib therapy and testicular hydrocele is evident by the fact that testicular hydrocele was repeatedly developed during imatinib therapy and improved after ceasing imatinib. The mechanism by which imatinib induces testicular hydrocele, however, is not clear, although it may arise through same mechanism of edema or fluid retention. Edema is the one of the most frequently reported adverse events, most of which are well tolerated. Unusual or severe cases of edema after imatinib such as cerebral edema, pleural effusion and severe periorbital edema were also reported (21-23). The mechanism of edema induced by imatinib is thought to be related with PDGFR. Signaling through PDGF-β receptors increases interstitial fluid pressure in the dermis (24, 25). On the contrary, inhibition of PDGF reduces interstitial hypertension and increases transcapillary transport in colonic carcinoma model (26). These studies suggested that the inhibition of PDGFR by imatinib is the possible mechanism of localized edema. Further investigation of the ability of imatinib to induce testicular hydrocele is warranted. To our knowledge, this is the first report of male gynecomastia and concurrent testicular hydrocele following imatinib treatment of a patient with GIST.
 XML Download
XML Download