

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Menopause is the cessation of the monthly hormonal cycle in adult women, and it results in decreasing estrogen levels and a lack of menstruation. Without folliculogenesis, the cystic activity in the ovary ceases. More than 80% of ovarian cancer occurs in women over the age of 50 yr. Older women are more likely to present with advanced disease, and their relative 5-yr survival rates are less than half of that for women that are under the age of 65 yr (1). The presence of even a relatively simple ovarian cyst in the postmenopausal woman is considered as ominous.
The standard operative approach for postmenopausal adnexal masses, whether they are detected by manual or ultrasound examination, has been exploratory laparotomy to rule out the possibility of ovarian malignancy (1). This approach has been adopted even though most adnexal cystic masses in these women are benign (2, 3). Operative laparoscopic techniques, because of their safety and efficacy, have been suggested as an alternate approach to open surgery for the treatment of adnexal masses in pre- and postmenopausal women (4, 5).
Several researchers have claimed that ultrasound can accurately predict benign cystic masses in the majority of postmenopausal women (6-8). Various sonomorphologic scoring systems that assign numerical ultrasonographic parameters to adnexal tumors have been developed in order to differentiate between benign and malignant neoplasms in pre- and postmenopausal women (9). Sassone et al. have assigned four morphologic characteristics to adnexal masses (inner wall structure, wall thickness, characteristics of the septa and echogenicity) according to the likelihood of finding a malignant tumor (8). Our center has used this scoring system for ultrasonography in all our patients to identify the malignant features of adnexal masses.
In addition, CA-125 is a commonly used tumor marker to differentiate benign masses from malignant adnexal masses, and it is also used for follow-up of patients with ovarian cancer. Serum CA-125 values are elevated in different gynecologic and nongynecologic cancers, and also for some benign conditions. The reference value of 35 IU/mL was based on the pioneering work by Bast et al. (10) who have reported that only 1% of apparently healthy women and 6.3% of women with benign disease had values above that level. As the reference value of CA-125 rises, the specificity and predictive value of CA-125 increases (11, 12). It is generally believed that the greater the CA-125 value, the greater the probability that an abdominopelvic mass is cancer (13). Bast et al. (10) have demonstrated that as the reference value increased to 65 IU/mL, the number of apparently healthy women decreased to 0.2% and the number of patients with benign disease decreased to 2.1%. The specificity at the cutoff serum level of 35 IU/mL is low and therefore, this test is probably followed by a number of unnecessary tests and finally by interventions for patients with an endometrial or inflammatory adnexal tumor. At the level of 65 IU/mL, the specificity is high and for these patients having a high level, only a few unnecessary tests and interventions might be undertaken (14).
Current research now involves defining the criteria that will aid surgeons in selecting those postmenopausal patients who are likely to have benign cystic masses. In this study, we have combined Sassone's scoring system for transvaginal ultrasound and a serum CA-125 assay (using 65 IU/mL as a cutoff level) for the preoperative selection of postmenopausal women likely to have benign adnexal cystic masses. We have also evaluated the effectiveness and safety of laparoscopic management of adnexal cystic masses in postmenopausal women.
MATERIALS AND METHODS
We retrospectively evaluated the hospital records of all consecutive patients over the age of 47 yr at the Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan University School of Medicine from January 1996 to May 2004 that had a preoperative diagnosis of adnexal cystic mass, and whose surgery was done laparoscopically. Postmenopausal status was defined as a woman older than 47 yr of age with at least 12 months of amenorrhea. All the postmenopausal women underwent a transvaginal examination within 6 weeks of their operation. Patients were selected on the basis of preoperative clinical examination, transvaginal ultrasonography and a serum level of CA-125. The indications for laparoscopic surgery were: 1) adnexal cystic masses in the benign range (4-8) of Sassone's scoring system for transvaginal ultrasonography (8); 2) lesions larger than 3 cm but less than 10 cm; 3) a serum level of CA-125 less than 65 IU/mL. All procedures were performed solely by the surgeons from the Division of Gynecologic Oncology, Samsung Medical Canter. Preoperatively, all patients understood and were informed of the need for possible laparotomy or other indicated procedures. Initially, upon visualization of the abdomen and pelvis, any fluid that was present was aspirated and sent for cytology. Next, a thorough evaluation was made of the pelvis and abdomen including the adnexa, peritoneal surfaces, liver, diaphragm, omentum and paracolic gutters, and any suspicious or abnormal-appearing areas were biopsied and sent to the pathology lab. All adnexal masses were placed into synthetic bags and subsequently removed through the suprapubic port to avoid intraperitoneal spillage of the surgical specimen and contamination of the abdominal wall during the removal process. If spillage did occur, thorough irrigation with sodium chloride or Ringer's lactate solution was carried out. Bleeding was controlled by unipolar or bipolar coagulation forceps, or sutures, as was appropriate. Suspected malignancies of the adnexa masses were sent for 'frozen' pathological examination at the time of the operation. If no malignancy was detected, no further evaluation was done. As a rule, any sign of malignancy demanded exploratory laparotomy with complete tumor staging.
RESULTS
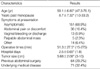
Operative laparoscopy was performed on 219 consecutive patients. The demographic characteristics of the postmenopausal women that were enrolled in our study are depicted in Table 1. Cesarean section was the most common previous history of abdominal operation, and this was followed by appendectomy, adnexectomy, tubal ligation, hysterectomy and nephrectomy, and the underlying medical diseases were most often hypertension, diabetes, thyroid disease, asthma, heart disease and renal disease. Laparoscopic management included, in the order of frequency, adnexectomy, oophorectomy, cystectomy and salpingectomy which was successful for 213 (97.3%) patients. Cystectomy was performed only for paratubal or paraovarian cyst. Among the 6 patients requiring laparotomy, five (83.3%) cases were converted electively at the discretion of the operating surgeon, and one (16.7%) case was converted based on the frozen section reports indicating a borderline ovarian malignancy that required staging laparotomy. Of the five cases electively converted to laparotomy, all these were due to the anticipated technical difficulties encountered because of extensive pelvic or extrapelvic adhesions.
The serum CA-125 levels were measured in all patients, and 10 (5.4%) patients had values between 35 and 65 IU/mL. The pathologic types of adnexal masses are shown in Table 2. Most of the adnexal masses were, in the order of frequency, serous cystadenoma, mature cystic teratoma, and mucinous cystadenoma. Among these 219 cases, one borderline ovarian malignancy was discovered on the frozen sections. The patient was 61 yr old and had a 5.5 cm-sized cystic mass in her right ovary with a normal CA-125 level (31.4 IU/mL). She also had surgical staging performed for ovarian malignancy and this revealed a borderline malignancy of serous cystadenoma on the permanent biopsy.
Intraoperative complications occurred in two patients due to bleeding from the secondary trocar entry site. Postoperative complications occurred in four patients due to superficial abdominal hematoma and a decrease in hemoglobin levels, but only one patient required a blood transfusion. There was no surgery-related mortality.
DISCUSSION
The aim of the current study was to evaluate the efficacy and safety of laparoscopic treatment for postmenopausal women with adnexal cystic masses that were predicted to be benign. The selection criteria used in this study were a combination of the Sassone's scoring system for transvaginal ultrasonography and the serum CA-125 level, and this combined criteria accurately predicted benign mass in most postmenopausal women (99.5%) except for only one patient who had a borderline ovarian malignancy. The laparoscopy was successfully completed in 213/219 (97.3%) patients without the need to proceed with laparotomy. Laparoscopic surgery for postmenopausal women resulted in shorter operative times and hospital stays compared to the conventional laparotomy procedure, and a history of previous abdominal surgery and underling medical diseases did not influence the success of laparoscopic surgery in these postmenopausal women.
With appropriate preoperative evaluation, laparoscopic surgery is well-known to be technically feasible, safe and advantageous with minimal morbidity, and this minimally invasive procedure could replace laparotomy for the management of most adnexal cystic masses occurring during the reproductive years (15-17). However, until now, the laparoscopic management of postmenopausal patients found to have an adnexal mass was controversial, although appropriate patient selection might be the critical factor for the successful application of this recently developed procedure.
The preoperative assessment by sonography for the size and consistency of an adnexal mass has been studied to determine the probability of malignancy (9). Most adnexal masses are benign (18), however, numerous studies have examined whether the gray-scale or Doppler sonographic criteria can allow for distinction between benign and malignant ovarian masses. When reviewing the entirety of the relevant literature, the studies indicate that no single gray-scale or Doppler sonographic feature allows for reliable distinction between benignity and malignancy. Despite the extensive literature on the subject that has been generated, the choice of which sonographic feature(s) to use, and in particular the role of Doppler sonography in predicting malignancy, remains controversial. Although most comparison studies have found gray-scale sonography to be superior to Doppler sonography (19-21), or that Doppler sonography offers no significant improvement over gray-scale sonography (22-24), a minority of studies have reported the Doppler features to be superior (25, 26). The Sassone's scoring system for ultrasonography used in our current study is a sonographic-morphological evaluation of adnexal masses using parameters such as the presence of papillary protrusions, solid parts, thick septa and high echogenic reflection patterns (8). These tumor morphology scores vary from 4 to 15, and a score of 9 was used to distinguish benign lesions from malignant tumors. Using a morphology score ≥9 as being indicative of cancer, malignant ovarian tumors were distinguished from benign lesions with a specificity of 83%, a sensitivity of 100%, a positive predictive value of 37% and negative predictive value of 100% (8). This scoring system seems to be extremely useful in assessing the risk of ovarian malignancy in postmenopausal women with adnexal cystic masses, and we have demonstrated this with the excellent results of our study.
Moreover, when we used the cutoff level of CA-125 as 65 IU/mL, there were 10 patients with the values between 35 and 65 IU/mL. In fact, the CA-125 level of one patient with borderline ovary tumor was below 35 IU/mL. As a result, the poor sensitivity and specificity of CA-125 limits its use as a sole screening test for early ovarian cancer. However, when the CA-125 level is elevated in association with an abnormal sonographic finding, and particularly in a postmenopausal woman, there should be a high index of suspicion for the presence of ovarian malignancy (9).
Several studies have reported on the safety and effectiveness of laparoscopic adnexectomy in postmenopausal women by using the selection criteria of ultrasonography and serum levels of CA-125. There was one study done on postmenopausal women having selection criteria for laparoscopy that included ovarian cysts that did not meet the criteria of a simple cyst, cysts were larger than 4 cm and had a pathological Doppler flow, or there was an elevated CA-125 level; all the laparoscopies were successfully accomplished and no cases of malignancy were found (27). In another study, when the adnexal cystic masses assessed by their transvaginal sonographic appearance were found to be other than a complex cyst, and this was paired with a normal serum CA-125 level, laparoscopic bilateral oophorectomy was performed in all 55 postmenopausal women and all the lesions were benign masses (28). There was another prospective multi-center study in which the selection criteria for the study were an adnexal mass evaluated with clinical examination, sonography, and CA-125 levels. The specific criteria included cystic masses greater than 3 cm but less than 10 cm, the masses had to have distinct borders without solid parts or septations greater than 2 mm, the patients were without ascites or matted bowel, and the serum CA-125 levels were less than 35 IU/mL. The final result was that all of the masses in the 61 postmenopausal women were accurately predicted to be benign (29). In this regard, we considered preoperative ultrasound examination and serum CA-125 level to be of utmost importance. Intraoperative frozen section examination is extremely helpful, although both sampling and judgment errors can and do occur in large borderline mucinous tumors (30).
In conclusion, by careful selection of patients using the Sassone's scoring system for transvaginal ultrasonography and the serum CA-125 assay (with 65 IU/mL as the cutoff level), laparoscopic management for postmenopausal adnexal cystic masses can be performed safely without fear of misdiagnosing the incidental malignant neoplasm, and this treatment method is technically feasible and safe with minimal morbidity.

 XML Download
XML Download