

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nonalcoholic fatty liver disease (NAFLD) is a clinicopathological syndrome characterized by hepatic steatosis with or without active inflammation (1) in patients with a negligible alcohol intake. There is growing concern about NAFLD, not only because this is a common liver disorder with a worldwide distribution, but also because it is recognized as one of the leading causes of chronic liver disease (2). In addition, a recent study has revealed that patients with nonalcoholic steatohepatitis (NASH) may progress to liver fibrosis, and approximately 8-17% progress to cirrhosis (2, 3). Although NAFLD may occur in non-obese patients (1), most cases of NAFLD are associated with obesity, type 2 diabetes mellitus (4), and hyperlipidemia (5). Weight reduction alone can improve liver function in obese patients with fatty liver (6). Moreover, insulin resistance underlies most cases of NAFLD, using the homeostasis model assessment-insulin resistance (HOMA-IR) method (7, 8), with a resultant increase in circulating insulin levels (9).
Adiponectin is a 30-kDa protein (10). In normal humans, its expression is restricted to adipose tissue (11). Plasma adiponectin levels are negatively correlated with the body mass index (BMI), fasting plasma glucose, fasting insulin, insulin resistance, and triglycerides (12). It is an anti-inflammatory adipocytokine that modulates insulin effects (13). The administration of adiponectin to mice decreased the plasma glucose (10), free fatty acid (FFA) and triglyceride levels (14), and hepatic glucose production (13). Plasma adiponectin levels are directly correlated with insulin sensitivity and, consequently, with decreases in obese and type 2 diabetic patients (11, 15).
Since adiponectin appears to induce insulin sensitivity, we hypothesized that hypoadiponectinemia is associated with NAFLD. Therefore, we investigated the relationship between NAFLD and plasma adiponectin levels and insulin resistance.
MATERIALS AND METHODS
The study subjects were recruited from participants in routine health examinations at the Department of Family Medicine, Korea University Hospital, Seoul, Korea, in February 2004. The study was approved by the ethics committee of Anam Hospital, and was conducted in conformity with the Helsinki Declaration. Written informed consent was obtained from all the participants before commencing the study.
One hundred and eighty one subjects were screened. After a standard interview (consumption of alcohol, medication, and disease history), forty four subjects who consumed alcohol more than twice per week, or more than 20 g per week, were excluded. Ten patients who had pathologic findings such as liver cirrhosis on ultrasound were also excluded. Sixteen subjects with evidence of viral hepatitis, toxic hepatitis, and serious cardiac, renal, or hepatic disease were excluded. Of the remaining subjects, after excluded elderly than seventies, 38 subjects with a 'bright liver' at ultrasonography were allocated as NAFLD group, while the 53 subjects with a 'normal liver' were assessed as control group.
Height (cm) and weight (kg) were measured to calculate body mass index (BMI) as weight (kg)/height (m2). Waist circumference was the minimum circumference between the costal margin and iliac crest. Body fat (%) was measured in a bioimpedance analysis (Inbody 3.0, Biospace, Seoul, Korea). Blood pressure was measured using a standard mercury sphygmomanometer, after the subjects were allowed to rest for at least 10 min.
Blood was obtained after a 12-hr overnight fast. A routine biochemical evaluation was performed, including serum aspartate aminotransferase (AST), alanine aminotransferase (ALT), total cholesterol, HDL-cholesterol, triglyceride, LDL-cholesterol, fasting plasma glucose, and fasting insulin. Serum was recovered from the supernatant after centrifuging it at 3,000 rpm for 15 min using a clinical centrifuge. The index of insulin resistance was measured using the homeostasis model of assessment (HOMA) method, as HOMA-IR (%)=fasting glucose/18× insulin/22.5, with insulin expressed in µU/mL and fasting glucose in mg/dL (16).
The adiponectin protein levels in human plasma were quantified using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (Quantikine) from R&D Systems (Minneapolis, MN, U.S.A.) after each serum sample was diluted 100-fold, according to the manufacturer's instructions.
All the subjects were given an ultrasound scan of the liver by an experienced radiologist who was blinded to the laboratory values. The diagnosis of fatty liver was based on abnormally intense, high-level echoes arising from the hepatic parenchyma, with amplitude similar to that of echoes arising from the diaphragm.
The results are expressed as the mean±SD for Gaussian variables and as median and lower and upper quartiles for non-Gaussian variables. Parameters that did not fulfill normal distribution (i.e., fasting insulin, HOMA-IR, adiponectin) were log-transformed for subsequent analysis. Anthropometric and metabolic characteristics for normally distributed data between control group and NAFLD group were compared by Student t-test and the Wilcoxon two-sample test for data not normally distributed according to sex.
Pearson correlation and partial correlation analyses were used to test the associations between plasma adiponectin levels and anthropometric and metabolic characteristics after adjusting for age, sex, and adiposity (BMI, waist circumference, and fat mass).
Multiple logistic regression analysis was used to determine the factors more closely associated with NAFLD, using the presence of NAFLD as the dependent variable, and adiponectin, BMI, waist circumference, HOMA-IR, age, and sex as independent variables. The level of statistical significance was set at p<0.05. All statistical analyses were carried out using the SAS computer analysis program (version 8.2; SAS Institute).
RESULTS
Anthropometric and metabolic characteristics of NAFLD and control groups in men and women, respectively, in Table 1. The study subjects were included 26 men and 65 women. The mean age was 51.3±8.8 yr and the mean BMI was 25.3±2.9 kg/m2. There was no significant difference in plasma adiponectin levels as well as other clinical parameters between control group and non-participants of this study. NAFLD subjects had significantly higher BMI, waist circumference, fat mass, fasting insulin, and HOMA-IR, and had significantly lower plasma adiponectin than control groups. Log levels of plasma adiponectin were significantly lower in men than in women (0.50±0.35 and 1.34±0.54, respectively, p<0.001).
Fig. 1 indicates plasma adiponectin levels and HOMA-IR in the NAFLD and control groups in men and women, respectively. Plasma adiponectin levels in NAFLD group were significantly lower than those in control group in both men and women. HOMA-IR in NAFLD group were significantly higher than those in control group in both men and women.
Fig. 2 graphically depicts the correlations of plasma adiponectin levels with HOMA-IR and waist circumference according to sex. Plasma adiponectin levels were significantly inverse correlated (r=-0.45, p<0.01) with HOMA-IR in women. In the other hands, the associations of plasma adiponectin levels with waist circumference was significantly inverse correlated in both men and women (r=-0.35 p=0.03, r=-0.41 p<0.01, respectively).
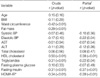
The univariate correlations and partial correlation analyses after adjusting for age, sex, and adiposity (BMI, waist circumference, and fat mass) between plasma adiponectin levels and anthropometric and metabolic parameters are shown in Table 2. Adiponectin levels correlated with waist circumference (r=-0.42, p<0.01), fat mass (r=-0.29, p<0.01), HDL-cholesterol (r=0.50, p<0.01), triglyceride (r=-0.31, p<0.01), and HOMA-IR (r=-0.34, p<0.01) in univariate analyses. Partial correlation analyses showed a significant positive correlation between plasma adiponectin levels and HDL-cholesterol levels (r=0.38, p<0.01). Conversely, negative correlations were observed between the plasma adiponectin levels and diastolic blood pressure (r=-0.22, p=0.04), triglycerides (r=-0.22, p=0.04), fasting insulin (-0.37, p<0.01), and HOMA-IR (r=-0.39, p<0.01).
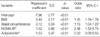
Table 3 shows the multivariate logistic regression analysis in which the presence of NAFLD was used as the dependent variable, while all variables were designated the independent variables. HOMA-IR indicative of insulin resistance, plasma adiponectin level, BMI, and waist circumference were independent factors significantly associated with NAFLD. The odds ratios for NAFLD with BMI (odds ratio [OR]=1.45; 95% confidence interval [CI]: 1.19-1.76), waist circumference (OR=1.13; 95% CI: 1.04-1.22), HOMA-IR (OR=2.38; 95% CI: 1.52-5.74), and plasma adiponectin levels (OR=0.22; 95% CI: 0.09-0.55) was statistically significant in multiple regression analysis that included all variables.
DISCUSSION
We found that the NAFLD group had a higher insulin resistance than the control group, which is in agreement with previous studies (17, 18). NAFLD is associated with insulin resistance and hyperinsulinemia in even lean subjects with normal glucose tolerance (18). It was suggested that insulin resistance is the pathognomonic condition responsible for NAFLD. Indeed, NAFLD is considered the hepatic manifestation of metabolic syndrome.
Insulin resistance is an essential requirement of NASH, independent of the degree of obesity (12). The insulin-sensitizing drugs troglitazone (19) and metformin (20) reduce aminotransferase levels. In the insulin-resistant state, accelerated lipolysis of adipose tissue results in an increased supply of hepatic free fatty acids (FFAs) and increased lipid oxidation, this is accompanied by fat accumulation in hepatocytes. There is a good correlation between the liver fat content and liver insulin resistance in normal subjects and in type 2 diabetic patients (20).
In this study, insulin resistance was measured using the homeostasis model assessment method, although euglycemic-hyperinsulinemic clamp is the gold standard for defining insulin resistance (7, 8). However, HOMA-IR is easy to perform, and that method is highly correlated with the euglycemic-hyperglycemic clamp (r=0.83, p<0.01) (21). The HOMA method for measuring insulin resistance has been applied extensively in epidemiological investigations (7, 8, 21).
Our study confirms that hypoadiponectinemia occurs in subjects with NAFLD, after controlling for age, sex, and adiposity. Animal models have indicated that adiponectin confers protective effects against alcoholic and nonalcoholic fatty liver disease (22, 23). Recent study reported that hypoadiponectinemia is a feature of NASH independent of insulin resistance and reduced adiponectin level is associated with more extensive necroinflammation and may contribute to the development of necroinflammatory forms of NAFLD (24). These data might also support the hypothesis that adiponectin has hepatoprotective effects in humans with NAFLD. The most likely reason for low adiponectin levels in NAFLD may be insulin resistance.
Our study found that HOMA-IR was significantly negatively correlated to adiponectin levels which were in accord with a previous report (25). Many investigators (8, 26, 27) suggest that adiponectin regulates hepatocyte metabolism directly. Long-term administration of adiponectin to diabetic mice improved the indices of insulin sensitivity, and decreased liver, muscle, and plasma triglycerides, and FFAs (22). Injection of recombinant adiponectin in mice increases fatty acid oxidation in muscle, reduces triglyceride content in muscle, and improves muscle sensitivity to insulin (14).
Raised plasma tumor necrosis factor (TNF)-α is thought to be another reason for the low adiponectin levels in NAFLD (28). Overproduction of the proinflammatory cytokine TNF-α by adipose tissue is involved in insulin resistance in obesity and TNF-α is a major cytokine contributing to liver damage in NAFLD (29).
In our study, plasma adiponectin levels were elevated more in women than in men. Similar results have been reported in several studies (29, 30), while others failed to observe a sex difference (31). The higher adiponectin expression in women, as compared to men, might be due to the fact that women tend to have less visceral fat tissue than subcutaneous fat tissue. Plasma adiponectin levels were determined predominantly by visceral fat, not by subcutaneous fat (32). Therefore, sexual dimorphism of the body fat distribution might contribute to the difference in plasma adiponectin levels in women and men.
Among the anthropometric index, waist circumference was stronger correlation with plasma adiponectin level, in our study. According to definition for metabolic syndrome suggested by the National Cholesterol Education Program Adult Treatment Panel III (33), abdominal obesity is one of the diagnostic criteria of the metabolic syndrome. Increased adiposity in the abdominal area may result in the development of insulin resistance, so abdominal obesity estimated by waist circumference, is inverse correlation with plasma adiponectin levels.
This study has some limitations. One limitation of this study is that the diagnosis of NAFLD was based on ultrasound examination, but was not confirmed pathologically. It is difficult to perform extensively in subjects with NAFLD, mainly for ethical reasons (34). Some prospective study comparing ultrasound scanning with histological examination indicated ultrasound scanning accurately identified steatosis with a sensitivity of 94% and a specificity of 84% (35). Recent study among biopsy proven NASH subjects also reported those patients had lower adiponectin levels and higher HOMA-IR than those with simple steatosis (24). Another limitation is that our study had a cross-sectional design, and there was potential bias in participation, so it cannot elucidate mechanisms or determine the direction of causality.
In conclusion, we demonstrated that hypoadiponectinemia and insulin resistance are associated with NAFLD independent of total heaviness and abdominal fat distribution. Adiponectin may be applicable in human disease as a novel agent for treating insulin resistance including NAFLD in the future. Further research is needed to identify the key determinants of circulating adiponectin and the development of NAFLD.



 XML Download
XML Download