

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The incidence of peripheral arterial disease (PAD) has increased in recent years owing to the aging of most populations and the increased prevalence of cardiovascular risk factors such as type 2 diabetes mellitus, obesity, and smoking in women (1). PAD is the most common manifestation of systemic atherosclerosis in which the arterial lumen of the lower extremities becomes progressively occluded by atherosclerotic plaques (2). The ratio of the resting ankle to brachial systolic blood pressure (SBP) provides an index (the ankle-brachial pressure index or ABI) that has been used widely in clinical and epidemiological studies to assess the patency of the lower extremity arterial system and to screen for PAD (3). The ABI has been associated with preclinical carotid plaques and the intimal-medial thickness (IMT) of the carotid and popliteal arteries (4, 5). A low ABI (<0.90) was reported to be a marker for risk of coronary and cerebrovascular disease (CVD) and was an independent predictor of CVD and allcause mortality (6, 7). PAD detected by means of the ABI has been associated with prevalent CVD and CVD risk factors in previous cross-sectional studies (8, 9). Moreover, many prospective studies have shown that a low ABI can predict CVD and all-cause mortality in general populations and in patients with existing vascular disease such as hypertension or type-2 diabetes mellitus, particularly in elderly men (10-12). A low ABI is common in elderly people and is accompanied sometimes by PAD. The prevalence of a low ABI varied from 3.0% in the Atherosclerosis Risk in Communities (ARIC) study (subjects aged 45 to 64 yr) to 19.1% in a study in Rotterdam (subjects aged 55 yr and older) (4, 13). Many community-based studies have been carried out in Western countries, whereas few epidemiological data are available from Oriental countries. In one study of elderly Japanese men (60-79 yr old), the prevalence of a low ABI was 5.0% (14), but, to our knowledge, there has not been an epidemiological study of a Korean population. Some clinical studies of ABI or PAD have included Korean subjects; however, these reports have limited significance because these studies were restricted to subjects with type-2 diabetes mellitus and renal failure (15, 16). Therefore, we conducted a community-based study to determine the distribution of ABI in Korean adults in order to provide baseline data for a prospective study.
MATERIALS AND METHODS
Populations and study design
Potential participants for this study were recruited from the inhabitants of five administrative regions (three Myuns and two Dongs) of Namwon in the Jeonbuk Province of Korea. We used national resident registration lists to identify potential participants, who were required to be 45-74 yr old in 2004. The study participants were selected randomly by cluster sampling in which sampling units were chosen at the smallest administrative district level, i.e., at the level of the Myun and Dong. The target area had an estimated 4,697 people (2,142 men and 2,555 women) that were of eligible age. All eligible people were invited, by means of a letter and a telephone call, for a medical checkup on a specific date at the Namwon Medical Center, Korea. All participants provided informed consent, and the study was conducted in accordance with the guidelines in The Declaration of Helsinki. The study was approved by the appropriate research ethics committee.
Among the 4,697 eligible subjects aged 45 and 74 yr, 1,964 (41.8%) underwent a clinical examination following an interview. The participants included 694 men and 1,270 women, and the mean (± standard deviation) ages of the men and women were 61.9±6.7 and 61.1±7.1 yr, respectively. The response rate of women (48.4%) was significantly higher than men (33.5%), but the difference of mean ages between the respondent and non-respondent was not significant in both sexes. ABI measurements could not be completed in the following 21 subjects (0.4%), who were excluded from the study: five subjects (24%) were in a post-operative state (leg surgery), four subjects (19%) could not assume a supine position for the examination owing to physical disability, two subjects (10%) had an artificial leg(s), and ten subjects (48%) had insufficient data to calculate the ABI. Ultimately, 1,943 subjects (41.4% of eligible subjects; 681 men and 1,262 women) formed the final study sample for the principal analysis.
The design of the study was cross-sectional and was based on the randomly selected community cluster samples (see explanation above). This is an ongoing prospective study that was designed to investigate the determinants of the occurrence and progression of CVD, osteoporosis, and dementia in elderly Koreans. This article represents an initial report of the first baseline examination of the cohort that is undergoing the prospective study.
Measurement of the ankle-brachial pressure index
The ABI was measured by experienced research staff and medical doctors according to a standardized protocol (2). Participants rested in the supine position for at least 5 min before measurements were made. Using a bidirectional Doppler (BiDop ES-100V) with a hand-held, 8-MHz probe (Koven Technology, St. Louis, U.S.A.) and a standard mercury sphygmomanometer (Baumanometer Kompak WA Baum Copiague, NY, U.S.A.), we measured systolic blood pressure (SBP) in the following order: right brachial artery; right dorsalis pedis and posterior tibial arteries; left dorsalis pedis and posterior tibial arteries; and left brachial artery. Arm cuffs of different sizes were used to accommodate different examinees.
If a discrepancy existed between both arms and between two arteries in the leg, the higher of the two SBP values was used to calculate the ABI. The ABI for each leg was calculated by dividing the highest value of either ankle SBP by the highest value of either brachial SBP. The lower of the two ABI values for the legs was used to define a low ABI value. ABI values were grouped into six categories: <0.90, 0.90-0.99, 1.00-1.09, 1.10-1.19, 1.20-1.29, and ≥1.30. An ABI value that was less than 0.9 was defined as a low ABI, while an ABI ≥1.3 was defined as a high ABI.
Measurement of cardiovascular risk factors
Anthropometric measurements of subjects that wore light clothing and were without shoes were conducted by experienced research staff. Height was measured to the nearest 0.1 cm, and weight was measured in the upright position to the nearest 0.1 kg. The body mass index (BMI) was calculated as weight divided by height squared (kg/m2). Waist circumference was measured to the nearest 0.1 cm at the end of a normal expiration by measuring from the narrowest point between the lower borders of the rib cage and the iliac crest.
Blood pressure was measured after 5 min of rest with the subject in the sitting position using a mercury sphygmomanometer (Baumanometer). The first appearance (phase I) and disappearance (phase V) of Korotkoff's sounds were used to define SBP and diastolic blood pressure (DBP) (17). Three readings each of SBP and DBP were recorded at intervals of 1 min, and the average of the three readings was used for the analysis.
All the participants underwent at least 10 hr of overnight fasting before blood samples were obtained from an antecubital vein. Serum was separated on-site and was stored at -70℃ until analyzed. Concentrations of total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), and triglycerides (TG) were measured by an automatic analyzer (AU5400, Olympus, Japan). The ratio of TC to HDL-C (TC/HDL-C) was calculated. The fasting blood glucose level was measured using an enzymatic method. The white blood cell count was quantified using a cell counter (Micros 60, ABX, Montpellier, France).
The presence of atherosclerotic plaques was recorded by a neurologist with the aid of a B-mode ultrasound sonogram (SonoAce 9900, Medison, Seoul, Korea). The site of plaques at any of the six segments of the carotid arteries was noted. Plaques with a wall thickness in excess of 1.5 mm were recorded, and the presence of lumen encroachment or an irregular intimal surface and/or image characteristics indicative of structural heterogeneity of the arterial wall were noted (18).
The questionnaire that was administered was designed to determine the history of CVD, type 2 diabetes mellitus, hypertension, and medication. Lifestyle questions included alcohol consumption habits, smoking habits, and exercise habits. Smoking habits were categorized as follows: current smokers, ex-smokers, and non-smokers. Subjects with persistent elevated blood pressure (≥140/90 mmHg) or who were on antihypertensive medication were classified as hypertensive according to the criteria of the report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) (19). Type 2 diabetes mellitus was defined as a self-reported history (being informed by a physician that diabetes was present) or as a fasting blood glucose level was equal or higher than 126 mg/dL according to the criteria of the American Diabetic Association (20).
Analysis
The demographic and clinical features of the study population are presented as the mean (± standard deviation) or a proportion according to sex. According to the ABI categorizations, age- and sex-adjusted mean values of CVD risk factors were calculated using an analysis of covariance (ANCOVA). The prevalence of CVD risk factors was analyzed using logistic regression models for heterogeneity. Overall difference and linear trends according to the ABI values were analyzed. As the distribution of TG was skewed, data were log-transformed prior to the analysis. All analyses were performed using SPSS software version 11.0 (SPSS, Chicago, IL, U.S.A.).
RESULTS
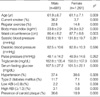
The demographic and clinical features of the study population are presented in Table 1. The percentages of smoking, regular exercise, high ABI, and the presence of carotid plaques were significantly higher in men than in women; the low ABI value was not significantly different between the sexes. The white blood cell count was not significantly different between the sexes, but the BMI was significantly greater in women. Triglyceride concentrations and fasting blood glucose levels were significantly different between the sexes, but SBP, DBP, and pulse pressure were not significantly different.
The distribution of ABI according to sex is presented in Fig. 1. In most subjects (-90%), the ABI was between 1.00 and 1.29. The most frequent ABI values in men were in the range 1.10-1.19 (42.4%), followed by 1.00-1.09 (29.4%) and 1.19-1.20 (19.7%). In women, the values with the highest frequency were in the range 1.00-1.09 (43.1%), followed by 1.10-1.19 (35.9%) and 1.20-1.29 (10.2%). The prevalence of a low ABI was 2.2% in men and 1.8% in women, and a high ABI was observed in 3.1% and 0.8% of men and women, respectively.
The ABI was inversely and significantly associated with age, SBP, and DBP in both sexes (Table 2, 3). The ABI was also significantly associated with the age-adjusted percentage of smoking and hypertension. In men, the waist circumference was positively associated with the ABI, whereas in women, the trend for the same parameters bordered on significance. In women, a decrement of pulse pressure was associated strongly with an increment in the ABI (p<0.001), but this was not the case in men. In men, a decreasing prevalence of carotid plaques and decreasing fasting glucose levels were significantly associated with an increment in the ABI (p<0.01 and 0.05, respectively), but this was not the case in women. BMI, TG, TC/HDL-C, and white blood cell count were not significantly associated with the ABI in either sex.
DISCUSSION
Ours is the first population-based study to investigate the ABI and to evaluate associations between the ABI and cardiovascular risk factors in middle-aged and elderly Koreans. The results of the present study revealed that the prevalence of a low ABI was 2.2% in men and 1.8% in women. These values are lower than the value of 5.0% reported previously for Japanese men aged 60 to 79 yr (14). Moreover, the ABI values in the present study were substantially different from those reported for Western populations, which vary from 2.4% (mean age: 54.5 yr) to 16.9% (mean age: 69.0 yr) in men and from 3.4% (mean age: 53.5 yr) to 20.5% (mean age: 71.7 yr) in women (4, 13). Such differences may result partly from different demographics, including differences in age, socioeconomic status, lifestyle, dietary habits, smoking habits, and physical activity. For example, in the present study there was a relatively smaller proportion of current and former smokers (data not shown), particularly women, than in previous studies (4, 7, 13). In addition, our study group comprised mainly farmers who were more likely to experience intense physical activity compared with the general population.
Despite the low prevalence of low ABI values in the present study, ABI values were associated significantly with cardiovascular factors after being adjusted for age in both sexes. The significant association between a low ABI and cardiovascular risk factors such as age, smoking habits, hypertension, SBP, DBP, obesity, serum glucose levels, and carotid plaques is consistent with the findings of previous studies. However, we did not find an association between ABI values and BMI, TG, TC, or HDL-C values, which is contrary to several previous studies (11, 13, 14, 21-23). This may be attributable to the limited statistical power that resulted from the low prevalence of low and high ABI values or to the relatively greater proportion of younger subjects in our study compared with subjects in other studies.
Cigarette smoking is one of the most important risk factors for PAD (24). In our study, the prevalence of current smoker was higher in low ABI and high ABI than other intermediate ABI values in both sexes. This U-shaped relationship between ABI values and the prevalence of current smoker is consistent with previous studies (7, 25), which showed that the associations of a high ABI with all cause and CVD mortalities was similar to those of a low ABI. Although the biological mechanism of the U-shaped relationships between ABI and mortality or CVD risk factors has not been fully elucidated, this finding is somewhat meaningful for CVD risk stratification by ABI values. In men, the prevalence of hypertension showed inverse associations with the ABI values similar to SBP and DBP, but in women, an inverted U-shaped association was observed. This discrepancy with sexes may be due to small number of men subjects, especially in two lowest ABI values.
Several hemostatic factors have received attention as potential markers of PAD, which suggests that the inflammation process plays an important role in atherosclerosis (26). In the present study, subjects of either sex with low ABI values also had high leukocyte levels, although this trend was not statistically significant. The relationship between atherosclerosis and inflammation should be investigated using more sensitive markers, such as highly sensitive C-reactive protein, plasma homocysteine, and fibrinogen.
The ABI is a simple, noninvasive, and inexpensive diagnostic test for lower extremity PAD, and the test-retest reliability of the ABI is excellent. In addition, the validity of the test for stenosis (≥50%) in the leg arteries is high; sensitivity is -90% and specificity is -98% (27). In the case of Korean, the accuracy of the automated blood pressure measurement was 88.8% for peripheral arterial disease defined using photoplethysmography (28). Approximately 5% of persons with PAD have a normal ABI, often because lower-extremity arteries are calcified, which elevates pressures artificially (29). The accurate diagnosis of PAD is important because it is an independent risk factor for CVD morbidity and mortality that is known to affect the functioning of the lower extremities and quality of life (30). Early identification of PAD before progression to advanced ischemia is also important, particularly in patients with renal insufficiency and diabetes (31). Therefore, the routine measurement of ABI in a primary care setting is recommended for groups that are generally at high risk of CVD, even though such patients may be asymptomatic. In order to effectively apply a screening method to detect asymptomatic PAD and to evaluate the risk of PAD, an optimal diagnostic cutoff ABI value is needed. Unfortunately, there is no consensus regarding the age-dependent distribution of ABI values, nor is there an optimal diagnostic cutoff point to define abnormal or high-risk groups in Korea. Community-based studies such as ours provide the data that are required to establish an optimal diagnostic cutoff point.
The present study has some limitations. First, because this study was cross-sectional, we were unable to determine whether cardiovascular risk factors were causally related to the ABI values. Second, we might have underestimated the prevalence of low ABI values owing to our reliance on volunteers. Third, the relatively small sample size prevented us from showing statistically significant associations where these may have existed between ABI values and risk factors. Finally, the response rate in our study was relatively low compared with that of similar surveys (13, 23).
In summary, our results revealed associations between low ABI values and cardiovascular factors, except for diabetes and lipid profiles. Therefore, a low ABI value may be a useful marker and predictor for CVD. In addition, the prevalence of a low ABI was lower than in previous studies of populations in countries other than Korea. However, more confirmative data that we used requires, which in turn requires additional complementary and prospective studies.



 XML Download
XML Download