

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Individuals with chronic disease suffer from life style disruption and difficulty with every day activities or interests (1-3). This is largely due to a devastating illness itself (e.g., pain, physical disability) but in part also due to treatment-related factors such as adverse effects (3). Devins and his colleagues termed this illness-induced lifestyle disruption as "illness intrusiveness" (4). It was suggested illness intrusiveness stands as a common underlying determinant of quality of life in chronic disease or a mediator of psychosocial impact of illness (3, 5).
They also developed a thirteen-itemed self-report scale called the Illness Intrusiveness Rating Scale (IIRS), which defines illness intrusiveness as lifestyle and activity disruptions that arise as a result of an illness and/or its treatment (4). Specifically, IIRS measures illness-induced interference in 13 life domains important to quality of life; health, diet, work, active recreation (sports), passive recreation (reading, listening to music), finances, relationship with partner, sex life, family relations, other social relations, self-expression/self-improvement, religious expression, and community and civic involvement (4). This scale has been widely used in a various population of chronic diseases including end-stage renal disease (4, 6), multiple sclerosis (5), rheumatoid arthritis (2), cancer (7), hyperhidrosis (8), lupus (9), and transplant population (10) and more recently in psychiatric disorders such as anxiety disorder (11), bipolar disorder (12), and sleep disorder (13).
Moderate to high reliability and validity of IIRS was reported through a number of studies (e.g., see review by Devins [3]). IIRS also showed a stable and common three factor solution across diverse patient populations further enabling its comparison among different disease groups (14).
Despite the rigorous attention in psychosomatic research and the degree of examination of the psychometric properties this scale has received, one area needing further evaluation is the cross-cultural adaptation of IIRS (14). Even the psychological instrument with excellent psychometric properties in the original language sometimes yields the poor construct validity in different language versions (15). To our best knowledge, French and Chinese language versions are currently being investigated but have not yet been published and a Korean version had been developed but its validity has never been tested (16).
In order to examine this issue, we developed a Korean version of IIRS and tested its cross-cultural adaptation through investigating construct validity (i.e., factor analysis, internal consistency, and correlation with other scores of functional disability and depressive symptoms).
MATERIALS AND METHODS
Subjects
Subjects were 712 outpatients diagnosed with a variety of medical diagnoses. Diagnostic distribution included sero-positive rheumatoid arthritis (46.5%); end-stage renal disease under current dialysis (14.5%), either peritoneal or hemodialysis; diabetes (13.1%); hypertension (11.7%); cancer (9.4%) and others (4.9%). The sample was predominantly women (65.6%), married (77.9%) and completed high school or higher education (62.5%). Mean age was 49.6 yr (SD=14.75) and mean duration of illness was 8.3 yr (SD=5.2).
All the patients were recruited from the outpatient units of the Department of Internal Medicine and Hospital for Rheumatic disease at Hanyang University Medical Center in Seoul during one month period. Research associates approached candidate patients after reviewing the medical charts for the above mentioned five diseases and obtained informed consent to participate in the survey. By convenient sampling, 827 patients were approached and 115 either refused to participate or did not complete the questionnaire, leaving 712 as a final sample. The study was approved by the ethics review board at the Hanyang University Medical Center.
Procedure
Subjects were asked to complete the Korean version of the IIRS (IIRS-K), Korean Health Assessment Questionnaire (HAQ) and the Korean version of The Center for Epidemiologic Depression Scale (CES-D). Cross-cultural validation data are available for HAQ (17) and CES-D (18). Additionally, clinical and socio-demographic information was obtained from the patients and their medical records.
Measures
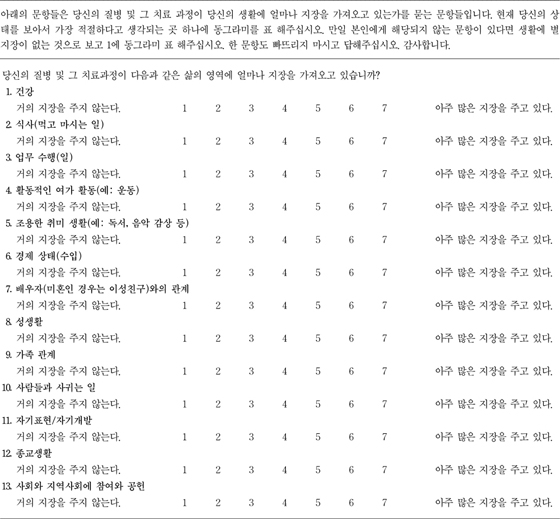
The IIRS captures 13 domains of everyday functioning and asks the respondents how illness or its treatment interferes with each domain. Respondents rate along a 7-point Likert scale, ranging from 1=not very much to 7=very much [4]. A total score can range from 13 to 91. Authors of this study agreed on a Korean language version (IIRS-K) after a translation and back-translation process.
Health Assessment Questionnaire (HAQ) (19), widely used self-rating instrument to measure functional disability in chronic illnesses and the Center for Epidemiologic Depression Scale (CES-D), a self-reporting depression scale composed of 20 items were also administered (20). Previous literature supports the association of IIRS total score with disability and depressive symptoms (2, 9, 21).
Statistical analysis
Initial factor structure of IIRS-K was examined by exploratory principle component analysis (PCA) with Varimax rotation in randomly split cases (n=356). This exploratory method was chosen because our objective of this study was to validate the Korean version of IIRS, although a three factor solution and its stability among diagnostic groups is known for original English version (4).
To further corroborate the stability of factor structure, remaining cases (n=356) were analyzed by confirmatory PCA with oblique rotation. Maximum likeliness factor analysis was also employed to test the goodness-of-fit of the model. We conducted Pearson correlation among total or factor scores of IIRS, HAQ and CES-D scores. Finally, we calculated the internal consistency of the items and factors. All data analyses were conducted using the Statistical Package for the Social Sciences (SPSS) 10.0 for Windows.
RESULTS
Exploratory factor analysis
Exploratory PCA with Varimax rotation in the exploratory sample (n=356) extracted two factors, of which the number was determined by size of eigenvalue, variance explained, and the scree test. Items with factor loading exceeding 0.40 and no cross-loadings were assigned to factors.
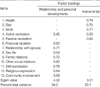
As shown in Table 1, Factor 1 labeled "Relationships and Personal Development" included eight items: financial situation, relationship with spouse, sex life, family relations, other social relations, self-expression/self improvement, religious expression, community and civic involvement. Factor 2, termed "Instrumental" included four items: health, diet, work, and passive recreation. This two-factor solution accounted for 57% of the total variance. Item 4, active recreation had cross loadings (0.40 or greater on two-factors) and was excluded for subsequent statistical analyses.
Confirmatory Analysis
As the two factors in exploratory analysis were intercorrelated (0.70), a confirmatory PCA with oblique rotation was used for the remaining half of the cases (n=356). The same two-factor structure was extracted. This result was replicated for total subjects (n=712). However, when we employ maximum likelihood factor analysis with oblique rotation to test the goodness-of-fit of the two factor model, statistically significant chi-square test resulted suggesting more factors are needed (χ2=138.2, df=43, p<0.001).
Reliability
We calculated reliability (alpha coefficient) of two subscales in the entire sample (n=712). The alpha coefficients for Relationships and Personal Development subscale were 0.89 and Instrumental 0.75. Each item of IIRS-K had coefficients ranging 0.48-0.74; total items 0.92. Thus, reliability was high for both factors and also for total items.
DISCUSSION
This study examined the factor structure of IIRS-K in a sample of chronic medical diseases, predominantly rheumatoid arthritis. Exploratory PCA and further confirmatory factor analysis extracted two factor structure, "Relationships and Personal Development" and "Instrumental". This result is comparable to original IIRS with three-factor solution; instrumental, intimacy, and relationships and personal development (14).
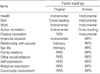
Overall speaking, more relational aspects were emphasized in the factor structure of IIRS-K when compared with the original IIRS (Table 2). For example, Intimacy (Item 7.8) in the original IIRS submerged in Relationships and Personal Development (Item 6-13) in IIRS-K. These two items (relationship with spouse and sex life) may be seen as a part of private and intimate sector distinct from relationship with others by North Americans, but Koreans may see that relationship and involvement with partners as a continuum of relations with others. This value of interdependence and harmony with others rather than individualism was described for Asians (22) and sometimes explained in the Confucian ideal (23).
Even Item 6, financial situation was loaded under factor "Relationships and Personal Development", not "Instrumental". It is not uncommon in Korea many patients with chronic illnesses depend financially on their family or relatives for medical expenditure because of incomplete coverage by medical insurance and welfare system. One research shows that Asian Americans are more likely to seek social support for their stress compared with European Americans (24).
Items on Instrumental (item 1, 2, 3, 5) of IIRS-K bear some differences to original Instrumental (item 1, 3, 4, 6). Item 2, diet had cross-loading and was excluded in IIRS but included in this study. Besides, Item 4, active recreation included as Instrumental in IIRS was dropped in IIRS-K. This item had cross loading on both Instrumental and Relationships and Personal Development. Koreans seem to foster more interpersonal aspects of exercises, which was shown as an example in the questionnaire. Item 5, passive recreation belonged to Instrumental, which was under Relationships and Personal Development in original IIRS. Once again, examples for passive recreation were reading and listening to music, which may be seen as mechanical and daily activities.
Therefore, we suggest that difference of factor structure from the original IIRS is in fact, reflection of cultural emphasis on relation with others and difference in life styles.
The limitation of corroborating two-factor solution in IIRS-K is that confirmatory maximum likelihood method failed to support the goodness-of-fit of the model. It generally means more factors are needed to account the structure but also may reflect sensitivity to sample size. Moreover, two factors had moderate to high internal consistency and correlated with disease characteristics (i.e., functional disability) and emotional distress (i.e., depression) well demonstrating the construct validity of two factors.
Other weakness of this study includes convenient sampling method and disproportion of diagnostic distribution may hazard the representativeness of the subjects. Taken together, these findings suggest construct validity of IIRS-K; however, corroborating two-factor solution needs further investigation. Likewise, we did not find cross-cultural equivalence of three-factor structure of IIRS.
 XML Download
XML Download