

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Catheter infection in the management of acute hydrocephalus could result in serious consequences such as intellectual deterioration and neurological deficits, including death in severe cases. Infection rates related with external drainage of cerebrospinal fluid (CSF) is reported as high as 4-17.2%, and efforts to reduce catheter-induced infection rates during CSF drainage have included intravenous antibiotics, local antiseptics, or lengthening of the subcutaneous catheter (1-3). All of these efforts during last two decades are still unsuccessful in significantly reducing catheter-induced infection (4-8).
It is very difficult to develop a polymer that releases antibiotics slowly to reduce catheter-induced infection rates, because the antibiotic ratio to catheter is limited to less than a few percent, resulting in the low concentration of releasing antibiotic (9, 10). This is because the released quantity of the antibiotic is variable with time, such as an initial burst, or terminal dumping effect of the antibiotic and also because the polymer usually does not endure heat up to 300℃ during the catheter molding process of the silicon (11, 12). Complexity of development of these antibiotic-releasing polymers was resolved with introduction of a simple coating and impregnation method of the catheter with antibiotics or antiseptics (5, 11-15). Coating of the silicon catheter is relatively simple, but still complex than impregnation of the catheter in methodology and safety (5, 16). The impregnation method is so simple and effective that some clinical trials have already been held and entered the commercial market, for the example, Bactiseal™ of Codman® (14, 16).
The authors of this study developed a basic polymeric structure applicable for a drug-delivery-system that had 1) a high drug composition of more than 10% in drug-polymer weight ratio, 2) easy control of the releasing rate by a minor change of the polymer structure, and 3) release duration of up to more than 6 months. Here we confirm the in vitro releasing characteristics and anti-bacterial activity, and suggest this to be new drug-delivery-system applied to CSF drainage catheter and others.
MATERIALS AND METHODS
Synthesis of polymer
Authors synthesized a new nalidixic acid polymer using diisopropylcarbodiimide, poly (e-caprolactone) diol, and nalidixic acid. Boiling temperature of the polymer was 350℃, and the white powder in room temperature. Depending on the amount of nalidixic acid, PCL-1250 and PCL-2000 were developed (Fig. 1). The synthetic process is summarized as follows: 1.16 g of nalidixic acid and 0.756 g of diisopropylcarbodiimide was dissolved in 40 mL of methylene chloride and stirred at room temperature for 1 hr. After 1 hr, 10 g of poly (caprolactone) diol (M.W.:1250) was added and stirred at room temperature for more than 24 hr. The solvent was evaporated, and the residue was dissolved in tetrahydrofuran and washed with 1 M NaOH. After drying under reduced pressure, the product was obtained (13). The authors evaluated the released monomeric structure, including nalidixic acid from nalidixic polymer, releasing rate, and anti-bacterial activity.
Structural validation with mass spectrometry and HPLC
Mass spectrometry (Agilent 1100 LC/MSD: LC solvent; Acetonitle: Ion polarity; positive: Ion source; APCI) was used to validate the structure of the released drug from the film associated with the cleavage sites in the drug polymer. Mass spectrometry was performed at 1 week, 3 weeks, and 6 weeks after the antibiotic polymer was immersed in 25 mL phosphate buffer saline (PBS; 0.1 M, NaCl; 0.138 M, KCl; 0.0027 M, Fig. 2). High pressure liquid chromatography (HPLC) estimated that releasing components were the polymer only, nalidixic acid, nalidixic polymer 1 week after in pH 7.4 phosphate buffer saline (NaCl 0.138 M, KCl 0.0027 M) and nalidixic polymer in chloroform (Fig. 3).
Releasing rate of nalidixic acid from nalidixic acid-loaded polymer
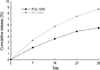
For the release study, the drug loaded polymer was immersed in 25 mL phosphate buffer saline (phosphate buffer; 0.1 M, NaCl; 0.138 M, KCl; 0.0027 M) containing 0.01 wt % NaN3. They were allowed to stand in thermostated shaking water bath at 37℃, 60 rpm. At each interval, the liquid phase was sampled for analysis, and the solvent in the tube was replaced with an equal volume of fresh buffer medium for the next release test. The amount of the released drug was measured at 330 nm with a UV visible spectrometer, and the cumulative release percent for each sample was calculated (Fig. 4).
Anti-bacterial activity of antibiotic-loaded polymer
The E. coli PI strain was grown in trypticase soy broth (Becton Dickinson Microbiology Systems, Franklin Lakes, NJ, U.S.A.) at 37℃ for 18 hr, and then adjusted to a concentration of 0.5 McFarland units (108 colony-forming units/mL) by using standardized spectrophotometric analysis. A cotton swab was dipped into the bacterial suspension and then rubbed in a streaking fashion across the whole surface of a Mueller-Hinton agar plate (Becton Dickinson Microbiology Systems, Franklin Lakes, NJ, U.S.A.). The 10 µL was taken from 30 mL of normal saline solution in which the drug loaded polymer (10 g) was immersed for a given period (every 2-4 weeks). After sampling, the whole saline solution was replaced with a fresh one, and the drug loaded polymer was immersed till the next sampling. The 10 µL taken from 30 mL of normal saline solution, in which drug loaded polymer (10 g) was immersed for a given period, was diluted four times with normal saline. Each diluted 10 µL was dropped softly onto the center of the agar plate that had been freshly inoculated with E. coli. After 10 µL drop was dried, the agar plate was incubated at 37℃ for 24 hr. The zone of inhibition was assessed by measuring the radius of the clear zone of inhibition on the given dilution ratio. The comparative anti-bacterial activity was calculated on the basis of first 5 days, from the ratio of dilution and the radius of zone of inhibition. Each cumulative antimicrobial activity was calculated from comparative anti-bacterial activities. This assay was performed every 2-4 weeks up to 16 weeks (Fig. 5).
RESULTS
Structural validation with mass spectrometry and HPLC
The mass spectrometry showed two high peaks (233.1, 274.0) demonstrating that the pure drug, nalidixic acid, and nalidixic acid salt were the major products of degradation and release. Early minor peaks of 90, 104, 127, 146, 174 might be the degraded products of the drug or oligomer, in which the cleavage sites are other than the ester linkage directly attached nalidixic acid. Several minor peaks larger than nalidixic acid (233) at about 7 days might be the drug loaded oligomer or degraded one (Fig. 3).
HPLC showed a peak at 5 min for nalidixic acid in PBS, and no peak within 30 min for polymer in PBS. It showed various peaks of less than 5 min and multiple overlapped peaks on 30 min for nalidixic acid loaded polymer in chloroform. It also showed a peak of nalidixic acid on 5 min for nalidixic acid loaded polymer in PBS for 7 days (Fig. 4). PCL-1250 and PCL-2000 showed the same results in the mass spectrometry and HPLC.
Releasing rate of nalidixic acid from nalidixic acid-loaded polymer
The cumulative amount of released nalidixic acid from the two drug-loaded polymer of PCL-1250 and PCL-2000 was calculated from the measurement with UV visible spectrometer, and showed 2.1 and 3.3% at 1 week, 3.6% and 5.7% at 2 weeks, 4.9% and 7.5% at 3 weeks, and 5.5% and 8.7% at 4 weeks, respectively (Fig. 5). The drug nalidixic acid was released from the drug-loaded polymer beyond 20% for about 40 days without initial burst effect.
Anti-bacterial activity of antibiotic-loaded polymer
When each anti-bacterial activity of the first 5 days for E. coli, Staphylococcus aureus, and Salmonella typhi was compared comparatively, each cumulative anti-bacterial activity of PCL-2000 for E. coli, Staphylococcus aureus, and Salmonella typhi was 5, 9, 2.4 during next 5 days, 7, 9.5, 3.5 during next 30 days, 15, 17.5, 26.9 during next 20 days, 31, 49.5, 73.5 during next 20 days, 32, 65.5, 78.5 during next 30 days, and 37.7, 88.4, 85.7 during the last 10 days (Fig. 6).
DISCUSSION
Bacterial infection is often a major complication to the more widespread application of polymeric materials in medical devices (17, 18). A foreign body such as a synthetic biomaterial causes the adhesion of microorganisms (18). The attachment of bacteria to a biomaterial surface has been known as a main factor in the initiation of biomaterial-related infections. Bacterial adhesion leads to their accumulation and production of extracellular polymeric substances. Bacterial growth in extracellular polymeric substances brings to the formation of the adhesive 'biofilms' and isolates the surface from the surrounding environment (19). The biofilms have been considered to diminish the activity of antibacterials, phagocytic cells, humoral antagonists and others (20, 21). Some general etiologic agents associated with biomaterial-related infections include Escherichia coli, Proteus mirabilis, Staphylococcus epidermidis, Enterococcus faecalis and Candida albicans (7, 13, 19, 22).
The bacterial growths with biofilms are able to resist several times of the lethal dose of the antibacterial agent (20, 23). Many approaches have been developed to make a biomaterial surface that has an antibiotic activity to reduce bacterial colonization and the formation of biofilm. Most of these approaches have been based on surface coating with drug or diffusion-limited systems for the delivery of the pharmacophores. Two most popular approaches are the coating of a device, such as a stent or catheter with antibacterial agents via an ionic bonding technique (25), and the impregnation of the silicon or urethane catheter with antibacterial solution via a simple dipping method of physical incorporation of the antibiotics in the polymer matrix (9, 11, 12). Other methods include the use of silver (25), and physicochemical surface modification (26-28). However, major problems in all these approaches were the fast or irregular release and the initial burst of antibacterial agents, leading to an erroneous infection during the contact (13, 15, 29).
Consequently, there has been a demand for a new method to prevent the adhesion of microorganisms. An alternative can be found in using the antimicrobial polymer that contains the antimicrobial agent linked covalently as a monomer into the backbone structure of the macromolecule. Woo and coworkers (10) studied a polyurethane copolymer synthesized using hexane diisocyante, poly (caprolactone) diol, a biodegradable polyester, and ciprofloxacin, a fluoroquinolone antibiotic. Their study showed that the degradable polyurethane, including the fluoroquinolone by covalent linkage, has an ability to destroy microorganism when released by degradation of polymer chains by the macrophage-derived enzyme cholesterol esterase. However, specification of the cleavage sites and releasing speed of the drug in the drug polymer were not easy to control (10, 15).
The authors of this study developed a new polymeric delivery system of slow releasing of drugs that has been never reported. New features of this delivery system might be that the drug is water soluble, but the matrix polymer and oligomers are not soluble in water. Since the drug-bounded oligomers are not soluble in water, the drug can be released only after the bound oligomers are degraded below a certain length. Also, the mutual compatibility between the matrix and the oligomer prevents the initial burst effectively. Practically, we could increase the drug-polymer ratio up to more than 10% very easily, and change the releasing speed of the drug to 10 months by controlling the water solubility (hydrophobicity) of the drug and polymer only, without any initial burst (data not shown). It is suggested that this delivery system could be applied to the drainage catheter and drug-delivery systems, for slow and continuous drug delivery probably such as anticancer agents or hormones.





 XML Download
XML Download