

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Congenital nephrogenic diabetes insipidus (CNDI) is a rare inherited disorder characterized by the insensitivity of the distal nephron to the antidiuretic effect of vasopressin. The defective urine concentration causes polyuria, hyposthenuria, nocturia, enuresis, functional obstruction and compensatory polydipsia. Patients with this disorder exhibit clinically recurrent episodes of hypernatremic dehydration, irritability, poor feeding, failure to thrive, constipation, and recurrent fever during infancy. Delayed diagnosis may lead to mental and physical retardation. The lack of response to exogenous vasopressin differentiates this disorder from central diabetes insipidus.
Although all types of CNDI share the same clinical features, three forms have been identified based on the inheritance pattern; the X-linked recessive form (OMIM 304800) associated with arginine vasopressin V2 receptor gene (AVPR2) mutations, and the autosomal recessive and dominant forms (OMIM 222000/125800) associated with aquaporin-2 gene (AQP2) mutations. About 90% of cases of inherited CNDI are X-linked. Autosomal recessive CNDI is much rarer and the autosomal dominant form is extremely rare (1).
In this study, we report on the clinical features of a Korean girl with CNDI and two novel heterozygous missense mutations in the AQP2 gene detected in her family.
CASE REPORT
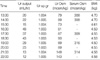
A 3-yr-old girl with a clinical diagnosis of nephrogenic diabetes insipidus was referred to the Department of Pediatrics, Seoul National University Children's Hospital for genetic studies. She was admitted to a hospital at the age of 1 month because of recurrent episodes of fever and hypernatremic dehydration. She had polyuria and polydipsia. At the initial evaluation, her hemoglobin was 16.5 mg/dL and hematocrit was 49%. Blood urea nitrogen and serum creatine were 8 mg/dL and 0.7 mg/dL, respectively. Serum sodium was 154 mM/L, potassium 4.7 mM/L, and chloride 124 mM/L. Serum and urine osmolalities were 328 mosm/kg H2O and 92 mosm/kg H2O, respectively. Serum arginine vasopressin level was 108 pg/mL (normal 4-12 pg/mL). Brain magnetic resonance imaging showed no abnormalities, and kidney ultrasonography revealed a large bladder with normal kidneys. The results of the water deprivation and desmopressin acetate stimulation tests were compatible with a diagnosis of CNDI (Table 1). Because the child was female without family history of this disorder, she was clinically diagnosed to have autosomal recessive CNDI, and the AQP2 gene analysis was performed.
Genomic DNA was extracted from the nucleated cells in the peripheral blood using a commercial kit (QIAamp DNA Blood Mini Kit, QIAGEN, Hilden, Germany). Each 4 exons with bilateral flanking introns of the AQP2 gene was amplified individually from the genomic DNA by polymerase chain reaction (PCR) and were directly sequenced. The sequences of the PCR primers were as follows; exon 1, sense 5'-CATCCTGGCCCTGAGACA-3', antisense 5'-GGATGGCAAAGTTGTGGC-3'; exon 2, sense 5'-CAGGAAGATGGAGCCAGAGA-3', antisense 5'-TGGAGTGGTCTGTGTGTCTG-3'; exon 3, sense 5'-GGACTTCCTGCCCTGTCC-3', antisense 5'-CCAGCTCTTGTTCTCCCT-3'; exon 4, sense 5'-GCAGCTGGCGTTGTCGTTGT-3', antisense 5'-TTCTGCCTCGGGCCTCACCC-3'.
Two heterozygous missense point mutations were detected in the patient; 70Ala (GCC) to Asp (GAC) in exon 1 inherited from her father and 187Arg (CGC) to His (CAC) in exon 3 inherited from her mother (Fig. 1). The former is located on the first NPA (asparagine-proline-alanine) motif of the aquaporin-2 molecule and the latter is located right after the second NPA motif.
She was treated with hydrochlorothiazide and amiloride, and her polyuria was partially relieved.
DISCUSSION
Almost all of the patients with X-linked recessive CNDI are male, and the exceptionally rare female patients, who are heterozygous for an AVPR2 mutation, are considered to have a skewed preferential inactivation of the X chromosome bearing the normal AVPR2 allele (2). Therefore, being a female in a patient with CNDI favors the diagnosis of the autosomal recessive or autosomal dominant inheritance rather than X-linked recessive inheritance. In addition, autosomal recessive or autosomal dominant CNDI can be differentiated from X-linked recessive CNDI by demonstration of a normal increase in the von Willebrand factor and factor VIII in response to exogenous vasopressin (3). Because vasopressin-induced increase in these coagulation factors is mediated by arginine vasopressin V2 receptor (AVPR2), this response is absent in patients with X-linked recessive CNDI having a defective AVPR2.
Recently, it has become possible in clinical practice to apply the direct analysis of the AVPR2 and AQP2 genes to the diagnosis and differential diagnosis of CNDI, because both genes are very short with 3 and 4 exons, respectively. This genetic diagnosis can be performed right after birth and even prenatally through chorionic villus sampling, amniotic cell cultures or cord blood sampling. Treatment with adequate hydration should be started as soon as possible after birth to prevent recurrent episodes of dehydration and a consequent permanent sequela of growth and mental retardation.
According to a literature review, we were able to identify 35 mutations of the AQP2 gene (4-8). Eight of these were associated with autosomal dominant CNDI (721delG, 727delG, E258K, 763-772del, 812-818del, 779-780insA, 756-765del, 812-816del) (4) and the remaining 27 with autosomal recessive CNDI. While the mutations causing autosomal dominant CNDI are centered around the C-terminus (CIV domain) of the AQP2 molecule, those causing autosomal recessive CNDI are widespread throughout the gene. Most of the former mutations are short deletions, while most of the latter are missense point mutations.
We found two novel heterozygous missense point mutations in this patient; A70D in exon 1 inherited from her father and R187H in exon 3 inherited from her mother. The former is located on the first NPA motif of the AQP2 molecule and the latter right after the second NPA motif. The NPA motif is one of the conserved sequences of aquaporins and several mutagenesis studies indicate that mutations near the NPA motifs alter aquaporin function (9), suggesting that this conserved region may be located at or near the water pathway. Besides, 187Arg is the site of a previously reported other functional mutation, R187C (10). Thus, either site of mutation is likely to be pathogenic, although we were unable to perform functional studies with A70D or R187H mutant.
AQP2 is a vasopressin-regulated water channel expressed predominantly in the principal cells of the collecting duct (4). AQP2 is selectively permeable to water molecules and is translocated between the apical membrane and subapical endosomes in response to vasopressin. Several pathogenetic mechanisms at a molecular level have been proposed to explain how an abnormal AQP2 decreases the water permeability of the cell. Some mutations in AQP2, particularly those affecting residues near the NPA motifs, produce functionally defective proteins (9). Some other mutations result in misfolding of the proteins. These misfolded proteins, which might be functional, are unable to move to the plasma membrane but are retained at the endoplasmic reticulum and rapidly degraded (4, 11, 12).
In several studies using transfected mammarian cells (11, 12), it was found that chemical chaperones such as glycerol can promote maturation and targeting to the plasma membrane of the misfolded proteins retained in the endoplasmic reticulum. Moreover, water permeability measurement in the cells demonstrated the occurrence of functional rescue.
These findings may be relevant to the development of novel pharmacotherapeutic strategies for CNDI. Unfortunately, however, the two mutations found in this patient are considered to produce functionally defective proteins because of their locations being at or near the NPA motifs. Therefore, these mutations are not likely to be rescued by chemical chaperones.
In conclusion, this is the first report to characterize AQP2 mutations associated with autosomal recessive CNDI in Korea, and expands the spectrum of AQP2 mutations by reporting two novel mutation, A70D and R187H.

 XML Download
XML Download