

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
CD30-positive anaplastic large-cell lymphoma (ALCL) is a rare subtype of non-Hodgkin's lymphoma that was described by Stein et al. in 1985 (1). The lymphoma usually occurs in lymph nodes, but the disease is known to involve various extranodal sites such as the skin (the most common site), and bone, lung, spleen and the gastrointestinal tract (2). In Korea, Cho et al. (3) have reported on multiorgan involvement of ALCL that included the stomach.
Primary gastric CD30-positive ALCLs are very rare, and there have been only a few such cases reported worldwide. Distinguishing gastric ALCLs from other the carcinomas or sarcomas may be confusing (2, 4, 5). Thus, a careful histologic examination for such cases is needed. We report here on a case of gastric Ki-1-positive ALCL that was proven pathologically. To the best of our knowledge, this is the first reported case of primary gastric ALCL in Korea.
CASE REPORT
In March 2004, a 50-yr-old woman was admitted to our hospital complaining of epigastric pain and severe anterior chest pain of 1 week duration. She was without any significant prior medical history. An electrocardiogram and an echocardiogram showed no significant abnormalities of the heart. We concluded that the chest pain was atypical and that it did not originate from the heart. Gastroendoscopic examination revealed a geographic mucosal irregularity at the antrum (Fig. 1A), and we performed a biopsy at the site. The pathology examination showed undifferentiated anaplastic neoplasm. Endoscopic ultrasonography showed the mucosal thickening (Fig. 1B), and the computerized tomography scan of the abdomen showed no evidence of distant metastasis. We performed follow-up gastroendoscopic examination after 2 weeks. The lesion was then more aggravated; her pain was persistent and did not respond to H2-blocker or proton pump inhibitors. She underwent total gastrectomy and the dissection of 16 regional lymph nodes.
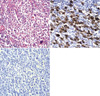
The gross finding of the resected stomach tissue revealed an 8×4.5 cm well-demarcated ulceroinfiltrative lesion at the pyloric antrum along the lesser curvature (Fig. 2), which infiltrated into the submucosal layer. There were many enlarged lymph nodes. The microscopic examination of the resected stomach tissue revealed a diffuse and solid proliferation of large atypical cells with pleomorphic nuclei. Some giant tumor cells were confined in the mucosa-submucosa area, and they showed multiple nuclear lobulations (Fig. 3A).
An immunohistochemical study was performed on the formalin-fixed, paraffin-embedded surgical specimens by the streptavidin-biotin-peroxidase complex method (LSAB kit; DAKO, Japan). The tumor cells were positive for CD30 (Fig. 3B), vimentin and CD3, but they were negative for cytokeratin, carcinoembryonic antigen (CEA), epithelial membrane antigen (EMA), CD45, CD20, CD45RO and anaplastic lymphoma kinase (ALK) (Fig. 3C). Eight of the sixteen lymph nodes contained metastasized tumor.
The patient had no B symptoms, and there was no bone marrow involvement. She had no palpable peripheral lymph nodes and there were no abnormal findings on chest radiography. The initial laboratory test results were as follows: white blood cell count, 4,300/µL; hemoglobin level, 10.3 g/dL; platelet count, 196,000/µL; lactate dehydrogenase level, 716 IU/L (240-460 IU/L). The serum calcium level, aspartate aminotransferase level and alanine aminotransferase level were normal. Her ECOG performance status was 1.
We diagnosed her as having CD30-positive primary gastric ALCL IIE, and we started chemotherapy with cyclophosphamide, adriamycin, vincristine and prednisolone. After two cycles of chemotherapy, prolonged leukopenia was noted. We then performed a bone marrow examination. The bone marrow revealed a hypocellular marrow (the cellularity was 10%) without evidence of tumor involvements. We decided to stop any further chemotherapy and the patient was closely followed up. At 7 months after diagnosis, the patient remains alive and without tumor recurrence.
DISCUSSION
The stomach is a common site of extranodal lymphoma occurrence, and most of the gastric lymphomas are of the B-cell type. Primary gastric CD30-positive ALCLs are very rare. There have been several previous reports regarding primary gastric ALCL in Japan and China (6-9); however, to the best of our knowledge, this is the first such reported case in Korea. We can only guess that it is indeed a very rare disease.
The ALCL cells are large and they have pleomorphic or multiple nuclei. Thus, primary gastric ALCL is sometimes misdiagnosed as undifferentiated carcinoma, melanoma, histiocytic neoplasm, sarcoma and so on (2, 4, 5). Unfortunately, we could not initially confirm the type of malignancy. The tumor cells of ALCL are CD30 positive and usually express EMA and one or more T-cell-associated antigens (1, 10). CD30 is a transmembrane cytokine receptor of the tumor necrosis factor receptor family. In the pathologic condition, it is expressed on the Reed-Sternberg cells of Hodgkin lymphoma and ALCL. CD30 is also observed in many categories of lymphoid tumors other than ALCL, and also can be expressed on embryonal carcinoma, however, the positivity of CD30 is usually weak in these cases. Other non-lymphoid malignant cells lack this CD30 expression. Although expression of CD30 is the hallmark of ALCL, it is not specific just for this disease. Therefore, it is necessary to perform other immunohistochemistry tests for other lymphoid and non-lymphoid markers (11). In our case, the tumor cells showed a similar morphology to those of ALCL. Immunohistochemically, most of the tumor cells were positive for CD30 and CD3, but negative for cytokeratin, CEA, EMA, thus confirming ALCL.
Anaplastic lymphoma kinase (ALK) expression is found in 50-70% of CD30-positive ALCL, and 75% of these cases have chromosomal abnormalities. ALCL is divided into three subgroups according to the ALK expression: ALK-positive systemic ALCL, ALK-negative systemic ALCL, and primary cutaneous ALCL (ALK negative). ALK-positive ALCL usually occurs at a younger age (15-30 yr), it is a male predominant disease, it exhibits frequent B-symptoms, it is known to be more chemosensitive and to have a better prognosis for survival (14, 15). However, Sachiko et al. have reported that one of three patients with gastric CD30-positive ALCL was positive for ALK and EMA (6). In our case, the tumor cells were negative for ALK immunohistochemistry, and the clinical characteristics of our case were in accord with the usual clinical findings for ALK-negative systemic ALCL.
Gastric T/null-cell lymphoma may be associated with Helicobacter pylori infection. Bariol et al. have reported gastric T-cell lymphoma regression with the eradication of H. pylori (9). In the present case, although we could not find H. pylori in the biopsy specimen, the urea breath test was positive. We performed H. pylori eradication with amoxicillin, clarythromycin and rabeprazole before obtaining the pathology results. However, the lesion became aggravated. Further study on the association between gastric T-cell lymphoma and H. pylori infection is needed.
Little is known about the treatment and prognosis of gastric ALCL. Most cases of gastric ALCL have been treated with surgical resection, and some patients have received chemotherapy after surgery. A few patients have received chemotherapy alone (12). The outcomes of treatment have been variable despite the different methods of treatment. Cases of primary gastric ALCL are very rare, so a standard treatment is not known. T-cell ALCL is generally an aggressive lymphoma, and Nakamura et al. have reported on rapidly progressive gastric ALCL (8). The treatment regimens for primary systemic ALCL are the same as those used for diffuse large B-cell lymphoma (13). Therefore, we performed chemotherapy with CHOP (cyclophosphamide, doxorubicin hydrochloride, oncovin [vincristine], and prednisolone) after the patient's total gastrectomy. After two cycles of chemotherapy, we were forced to stop the treatment because of the poor bone marrow reservoir. At 5 months after diagnosis, the patient is alive and there has been no tumor recurrence.
We can suggest that ALCL should be considered among the cases of pleomorphic tumors of the stomach.


 XML Download
XML Download