

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Osteoporosis is characterized by low bone mass and the microarchitectural deterioration of bone tissue with a consequent increase in bone fragility and susceptibility to fracture (1). The diagnosis and the clinical management of osteoporosis have been based on the measurement of bone mineral density (BMD) using dual X-ray absorbtiometry (DXA) as a standard method. However, BMD measurements alone do not provide information about the microarchitecture or the mechanical properties of bone. Quantitative ultrasound (QUS) methods have been introduced in recent years for the assessment of the skeletal status in osteoporosis. It has been suggested that QUS may provide information about not only bone density but also the microarchitecture and elastic properties of bone (2). The QUS measurements of bone status have been shown to be related to fracture risk, independently of BMD (3-5). However, calcaneal QUS thresholds for the diagnosis or treatment of osteoporosis have not as yet been defined. In addition, there are several unresolved issues concerning the accuracy, long-term stability and precision of the technique, cross-calibration between the various QUS devices (6).
In 1994, the World Health Organization (WHO) proposed guidelines for the diagnosis of osteoporosis based on BMD measurements. According to the WHO criteria, osteoporosis is defined as a BMD of 2.5 or more standard deviations (SD) below the peak mass of a young, healthy, sex - and race-matched reference population (7). However, the reference range may vary in different populations (8-10). Therefore, the construction of reference ranges that accurately represent the population at large is essential for the correct identification of osteoporosis.
The number of QUS devices in clinical use is scheduled to increase in Korea. However, there are currently no QUS reference data available for Korean population. This study aimed to establish reference data for the QUS measurements of the calcaneus and for the BMDs of the forearm and calcaneus, and to examine the correlations between the QUS parameters and the BMD in a Korean population.
MATERIALS AND METHODS
Subjects
The study population was composed of participants in the Namwon Study and the Thyroid Disease Prevalence Study. Out of 4,697 eligible subjects aged 45 to 74 yr in the Namwon Study which is an ongoing prospective study that was designed to investigate the determinants of the occurrence and progression of cardiovascular disease, osteoporosis, and dementia in elderly Koreans, 1,964 subjects (41.8% of eligible subjects; 694 men and 1,253 women) underwent clinical examinations following interviews. Out of the Thyroid Disease Prevalence Study participants, 3,000 subjects aged 20 to 74 yr were randomly selected by 5-yr age strata and sex from the Yeonggwang and Muan counties in Jeollanam-do province of Korea. Of these, 1,175 subjects (39.2% of eligible subjects; 575 men and 600 women) underwent clinical examinations. In all, a total of 3,139 subjects (1,269 men and 1,853 women) aged 20 to 74 yr were recruited. Of these, 3,053 subjects who underwent both QUS and BMD measurements (1,225 men and 1,828 women; 20 to 74 yr old) formed the final study sample for the principal analysis. All participants provided informed consent, and the study was approved by the institutional research ethics committee.
Anthropometric measurements
Anthropometric measurements of subjects wearing light clothing and no shoes were conducted by experienced research staff. Height was measured to the nearest 0.1 cm, and weight was measured in the upright position to the nearest 0.1 kg. The body mass index (BMI) was calculated as weight divided by height squared (kg/m2).
Measurement of risk factors
The questionnaire administered to all participants was designed to determine the history of type 2 diabetes mellitus, hypertension, medication and lifestyle factors such as alcohol consumption and smoking habits. For women, information on menstrual status and use of hormone replace therapy was also collected. The subjects were categorized according to their smoking habits as current smokers, ex-smokers, and non-smokers. Type 2 diabetes mellitus was defined as a self-reported history (having been informed by a physician that diabetes was present) or as a fasting blood glucose level ≥ 126 mg/dL. Subjects with persistent elevated blood pressure (≥ 140/90 mmHg) or who were on antihypertensive medication were classified as hypertensive according to the criteria of the report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) (11).
Measurements of quantitative ultrasound and bone mineral densitometry
The QUS parameters of the right calcaneus were determined in all participants using the Achilles InSight ultrasonometer (GE Lunar Corporation, Madison, WI, U.S.A.), according to the instruction manual provided by the manufacturer. Two QUS parameters were measured: broadband ultrasound attenuation (BUA) and speed of sound (SOS). A third parameter, the stiffness index (SI), was calculated using the formula, SI=(0.67×BUA)+(0.28×SOS)-420. The within-day coefficients of variation (CV) for duplicate measurements in 30 adults were 1.93% for SI, 1.74% for BUA, and 0.20% for SOS. The bone mineral densities (BMD; g/cm2) of the right calcaneus and the nondominant forearm were measured by dual energy X-ray absorptiometry (DXA) using a PIXI densitometer (GE Lunar Corporation). Calibration was performed daily with a physical phantom. The within-day CV for duplicate measurements in 60 adults were 0.19% and 0.17% for the forearm and calcaneus BMD, respectively.
Statistical analysis
Data are expressed as means±standard deviations (SD). The correlations were examined using Pearson's correlation and partial correlation, with age held constant. The T-scores for each subject were calculated using the means and SDs for the QUS parameters and BMD using the 20-39 age group in this study as the normal young adult comparison population. All analyses were performed using SPSS software version 11.0 (SPSS, Chicago, IL, U.S.A.).
RESULTS
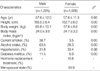
The demographic and clinical features of the study population are presented in Table 1. The mean ages of the participants were 57.6±12.0 yr for the men and 57.6±11.3 yr for the women. The percentages of smoking, alcohol intake, and diabetes mellitus were significantly higher in men than in women; the percentage of hypertension was not significantly different between the sexes. In women, the percentages of menopause and use of hormone replacement therapy were 64.9% and 10.8%, respectively.
Table 2 and 3 present the reference data for the QUS and BMD values according to age and sex for the population. The peak mean values for the QUS parameters occurred in the 20 to 29-yr-old subjects of both sexes, with the exception of the BUA, which reached the highest values in women of 30-39 yr. For both sexes, the mean BMD of the calcaneus was the highest in 20 to 29-yr-old subjects and that of the distal forearm was the highest in 40 to 49-yr-old subjects. From the peak values to the values in the 70 to 74-yr-old group, there were overall declines of 10.5% for BUA, 1.9% for SOS, 17.1% for SI, 23.4% for forearm BMD, and 24.2% for calcaneus BMD in men, and 20.8% for BUA, 3.1% for SOS, 31.6% for SI, 37.6% for forearm BMD, and 41.6% for calcaneus BMD in women.
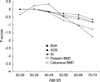
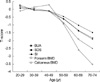
The mean ages of the young normal controls were 31.1±6.1 yr for the men (n=127) and 31.7±5.6 yr for the women (n=164). The means and SDs for the BUA, SOS and SI were 121.3±15.6 dB/MHz, 1,555.2±43.2 m/sec and 96.2±20.7, respectively for the men, and 113.7±13.8 dB/MHz, 1,551.0±29.1 m/sec and 90.0±15.4, respectively for the women. The means and SDs for forearm and calcaneus BMD were 0.589±0.071 g/cm2 and 0.623±0.113 g/cm2, respectively for the men and 0.496±0.052 g/cm2 and 0.493±0.081 g/cm2, respectively for the women. The age-related declines in T-scores for both the BMD and QUS measurements are shown in Fig. 1 and 2. The mean T-scores for the BMD measurements were more negative than those for the QUS measurements. In the 70-74 yr group, the mean T-scores for BUA, SOS, SI, forearm BMD, and calcaneus BMD were -0.8, -0.6, -0.8, -1.7, and -1.3, respectively, in men, and -1.7, -1.5, -1.8, -3.4, and -2.4, respectively, in women.
Table 4 shows the correlations between the QUS parameters and the BMD results. The correlations between BUA and SOS were found to be 0.69 in men and 0.61 in women. The correlations between the QUS parameters and BMD were 0.41 to 0.73 in men and 0.51 to 0.76 in women. The highest correlations were found between SI and calcaneus BMD in women (r=0.76) and between BUA and calcaneus BMD in men (r=0.73). The correlations between the BMDs of the distal forearm and the calcaneus were found to be 0.63 in men and 0.74 in women.
DISCUSSION
This study provides population-based reference data for the QUS parameters and the forearm and calcaneus BMDs in a Korean population. This is the first large study to present reference data for QUS parameters in both sexes in Korea. Kim et al. (12) presented reference data for the QUS of the calcaneus from 552 Korean women and 238 young women. Their data showed lower mean values for both normal young women and for women over 50 yr old, compared with the data presented here. When compared with the reference values reported in a Japanese study (13), our BUA data values were similar for both sexes, and our SOS data were similar for the 20-29 age group of men and the 20-39 age group of women; however, our SOS values for men over 30 yr and for women over 40 yr were higher than the Japanese values. The data values in the present study were lower than those reported in Brazilian women (14). The SOS data values in the present study were similar to and the BUA data were lower than the reference data reported for Nigerian women (15).
Shin et al. (16) presented the mean BMD values for a total of 317 healthy Korean women and 183 healthy Korean men aged 20 to 29 yr. The authors reported mean and SD values for calcaneus BMD in young males and females of 0.613±0.100 g/cm2 and 0.494±0.076 g/cm2, respectively; the values for forearm BMD in young males and females were 0.550±0.064 g/cm2 and 0.465±0.061 g/cm2, respectively. These values are lower than those in the present study; however, our data were similar to the reference values for Asia supplied by the manufacturer of the densitometer (0.580±0.06 g/cm2 for the forearm and 0.620±0.09 g/cm2 for the calcaneus in men; 0.490±0.06 g/cm2 for the forearm and 0.500±0.08 g/cm2 for the calcaneus in women).
In our study, the mean BMD of the distal forearm was the highest in 40 to 49-yr-old subjects. This finding is in accordance with previous studies (17, 18), but three large population studies (19-21) showed that the mean BMD of the distal forearm was highest in 30 to 34-yr-old subjects. This may be attributable to the ethnic difference or to use of the different devices to determine the BMD at the forearm. This also may be attributable to the relatively small sample of normal young adults in our study.
The age-related declines in the T-scores based on the QUS parameters were approximately half those based on the BMD measured by DXA. This is consistent with other studies (22, 23). When the WHO definition of osteoporosis is applied to the T-scores based on QUS measurements, the prevalence of osteoporosis appears to be lower than that determined based on BMD measurements. It is clear that the T-score cannot be used interchangeably with measurements derived from different techniques and different sites (24). Frost et al. suggested that the WHO T-score threshold of -2.5 for the diagnosis of osteoporosis requires modification when using QUS to assess the skeletal state and that a T-score threshold of -1.8, based on the BUA and SOS of the calcaneus, may be appropriate for identifying postmenopausal women at risk for osteoporosis (22).
In this study, the correlations between QUS parameters and BMD measurements were found to be 0.41 to 0.73 in men and 0.51 to 0.76 in women. The correlation coefficients between the QUS parameters and BMD values reported in other studies have ranged from 0.14 to 0.88, with most studies finding correlations in the range of 0.4 to 0.7 (25), suggesting that a considerable part of the variabilities of QUS and BMD are unrelated. The very high correlations we found between BUA and calcaneal BMD, and between SI and calcaneal BMD, with coefficients ranging from 0.71 to 0.76, were similar to those in other reports (26-28) because of same measurement site (25). The SI parameter, which had a high correlation with BMD in this and other studies, has been previously proposed by the manufacturer as a useful means of improving the correlation between QUS and BMD measurements.
The present study has some limitations. First, the response rate in our study was relatively low. However, because the sample size is sufficiently large, we believe the data are representative of the local population. Second, the relatively small sample of normal young adults prevented us from determining the young adult mean and SD representative of the Korean population. Thus, further larger studies are required to validate our findings.
In summary, we present data for the QUS and BMD measurements in a normal Korean population that can serve as reference data for studies examining the QUS of the calcaneus and the BMD of the forearm and calcaneus. Our result suggest that WHO T-score threshold of -2.5 for the diagnosis of osteoporosis requires modification when using QUS, and further larger studies are required to establish diagnostic threshold for QUS and peripheral DXA.



 XML Download
XML Download