

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spinal muscular atrophy (SMA) is one of the most common autosomal recessive disorders characterized by progressive muscle weakness caused by degeneration of the spinal anterior horn cells. SMA has a prevalence of 1/6,000 to 1/10,000 births and a carrier frequency of 1/40 to 1/50 (1-3). According to age of onset and severity of symptoms, patients with SMA are subdivided into three clinical types (4). Type I (Werdnig-Hoffmann disease; OMIM 253300) is the most severe form with the onset at birth to the first few month and death by 2 yr of life. Type II (OMIM 253550), intermediate form, is characterized by the onset before 18 months of age and survival beyond 4 yr-old age. Type III (Kugelberg-Welander disease; OMIM 253400) is the mildest form with the onset after the age of 2 yr and survival into adulthood.
All types of SMA are associated with homozygous deletion in the survival motor neuron 1 gene (SMN1; OMIM 600354) (5). SMN1 and its homologous gene, SMN2 (OMIM 601627), are located on 5q13. The two SMN genes are different at only five nucleotide exchanges within their 3' ends (5, 6). In contrast to SMN1, the expression of SMN2 protein is truncated from skipping of exon 7 by a single nucleotide exchange (840C→T) (7, 8). Approximately 94% of SMA patients lack both copies of SMN1 exon 7 (9), which can be detected by the commonly used molecular analyses (2, 10).
As the carrier frequency in population is high, the carrier test for SMA is important issue in genetic counseling. Until now, several quantitative PCR methods for SMN1 analysis have been developed for carrier detection (11-14). However, these methods were intricate and easily submitted to errors. Recently reported quantitative real-time PCR assays (15, 16) allow the specific amplification of only SMN1 gene, and become powerful tools to avoid these problems. However, these tests include still several limitations in relation to the specificity, and cost-effectiveness.
In consideration of these defects, we developed a reliable quantitative real-time PCR method using SMN1 gene specific primers and SYBR Green I dye for the carrier detection of SMA. The comparative Ct (threshold cycle) method was used to quantify the copy numbers of SMN1 gene. This test allowed us to analyze a large number of samples efficiently. Here, we report the results of quantitative analysis of SMN1 gene in SMA patients and parents, and the estimated carrier frequency in Korean population.
MATERIALS AND METHODS
Subjects
Quantitative analysis of SMN1 gene was done in 13 patients with SMA and their 24 parents. Clinical diagnosis was fulfilled on all patients and homozygous absence of SMN1 exon 7 was confirmed with polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) (2, 10).
To estimate the carrier frequency in Korean population, we selected 326 unrelated healthy individuals aged 19-81 yr who participated in a comprehensive health screening in Ansan Health Center (17). Informed consents for DNA analysis were obtained from the patients and normal individuals.
DNA extraction
Genomic DNA was extracted from peripheral blood samples by the QIAamp DNA blood kit (Qiagen, Hilden, Germany) and was measured by an Ultrospec®2100 (Amersham Pharmacia Biotech, Piscataway, NJ, U.S.A.). Samples that had purity in the range of 1.5-1.8 (260 nm/280 nm ratio) were used for highly efficient amplification. DNAs were diluted to a final concentration of 2.5 ng/µL.
Quantitative real-time PCR of SMN1
The quantitative real-time PCR assay was based on primers that specifically amplify SMN1 gene. To distinguish SMN1 from SMN2 (GenBank AH006635) in the amplication reactions, 3' ends of the primers were designed to end on the SMN1 specific sequence in exon 7 at position 6 and intron 7 at position +2: forward primer is 5'-CCTTTTATTTTCCTTACAGGGTTTC-3'; reverse primer is 5'-GATTGTTTTACATTAACCTTTCAACTTTT-3'. Specificity of the SMN1 primers was confirmed by multiplex PCR with COL1A1 gene (forward primer, 5'-GGGGGAACAAGGCTGTCT-3'; reverse primer, 5'-TCCTGGGGTTCAGACCAA-3') in patient samples and a normal individual's. As a reference gene, we used exon 12 of human serum albumin: forward primer is 5'-AGCTATCCGTGGTCCTGAAC-3; reverse primer is 5'-TTCTCAGAAAGTGTGCATATATCTG-3'. Using the ABI PRISM®7700 Sequence Detection System (PE Applied Biosystems, Foster City, CA, U.S.A.), the PCR was performed in a total volume of 20 µL in each well, containing 10 µL of SYBR Green® PCR Master Mix (PE Applied Biosystems), 20 ng of genomic DNA (8 µL), and 0.1 µM and 0.5 µM of SMN1 and albumin primers, which was determined after the analysis of the optimal concentrations of each primer. Each sample was run in triplicates in separate tubes to permit quantification of the SMN1 gene normalized to albumin. The PCR condition consisted of initial denaturation step of 95℃ for 10 min, followed by 40 cycles of 95℃ for 15 sec and 60℃ for 1 min.
Data analysis
All data were calculated by the comparative Ct method, to detect the relative gene copy numbers (18). By using a calibrator sample of a normal control DNA, the gene copy numbers of unknown samples were estimated. Patients, carrier, and unrelated normal samples were analyzed together with the calibrator sample on every assay plate. ΔCt represents the mean Ct value of each sample and was calculated for SMN1 and albumin. The gene copy numbers of the samples were determined by the following formula: ΔΔCt=[ΔCt albumin (calibrator sample)-ΔCt SMN1 (calibrator sample)]-[ΔCt albumin (unknown sample)-ΔCt SMN1 (unknown sample)]. The relative gene copy numbers were calculated by the expression 2-ΔΔCt. Using this method, a ΔΔCt ratio, [2-ΔΔCt], was expected to be about 1 in normal controls, about 0.5 in carriers and 0 in patients with SMA.
RESULTS
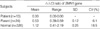
The Ct values of SMN1 and albumin triplicates showed almost identical at the amplification plots of a normal control (Fig. 1A). The standard deviations of triplicate Ct values for all samples were very low (mean, 0.10; range, 0.00-0.32). In parents of SMA patients, carrying only one SMN1 gene copy, the Ct values of SMN1 increased about 1.32 compared with albumin (Fig. 1B). In the SMA patients, the albumin gene was amplified as in normal controls, but the SMN1 gene was not amplified as expected (Fig. 1C). Their ΔΔCt ratios were 0.00 showing homozygous absence of SMN1 gene. In accordance with this result, there were no visible products of the SMN1 genes in SMA patients by multiplex PCR with COL1A1 gene (Fig. 2). The range of measured ΔΔCt ratios in 24 parents was between 0.39 and 0.59 (Table 1). To estimate the frequency of carrier in general population, we tested 326 healthy individuals. Among them, ΔΔCt ratios of 7 persons were within the carrier range, 0.41-0.57, indicating that the carrier prevalence was about 1/47 in Korean population (Table 2). The others were detected between 0.84 and 2.19. This result was classified into three groups according to the expected copy numbers of SMN1 (Table 2).
DISCUSSION
SMA carrier test based on direct quantitative analysis of SMN1 gene is one of the most important issues, since homozygous deletion of SMN1 exon 7 is a common variant. However, the reports of SMA carrier frequency have been concentrated in western countries (3, 11). Therefore, we tried to calculate the SMA carrier frequency in Korea and developed the reliable quantitative test of SMN1 based on real-time PCR with the SYBR Green I dye using the comparative Ct method. We used primers ending on to the nucleotide exchanges between the SMN1 and SMN2 genes in exon 7 to distinguish the SMN1 and SMN2 genes. The specificity and sensitivity of the test are 100%, although the presence of two SMN1 copies per chromosome or intragenic point mutations in some of the SMA chromosomes (approximately 5%) slightly decreases the sensitivity of the test.
We determined the range of carrier gene dosage in 24 parents (0.39-0.59) of SMA patients, in which homozygous deletion of SMN1 gene were identified previously by PCR-RFLP (Table 1), and then screened 326 healthy normal individuals. As shown in Tables 1 and 2, there is no overlap between the range of ΔΔCt ratio measured SMN1 copy numbers in carriers and normal individuals. The prevalence of carrier was 1/47 in Korean population (95% confidence interval: 1/175-1/27), within the similar ranges reported in western countries (1, 3, 11). In 65 individuals, the SMN1 copy numbers were three or four copies like as in other countries (11-13).
Since SMA is a fatal disease, coefficient of selection of SMN1 deleted homozygotes is almost one. Therefore, extrapolation of Hardy-Weinberg equation to calculate the prevalence of SMN1 deleted homozygotes in a population seems to be unreasonable. Nevertheless, if ignoring this potential bias, the disease prevalence of SMN1 deleted homozygotes calculated by Hardy-Weinberg equation was 1/8,496 in Koreans. The estimated prevalence was also not much different from those of other European countries. Since there was no available information of SMA prevalence in East Asian countries including Korea, estimated prevalence presented in this study would be valuable for pursuing SMA pathogenesis and genetic counseling.
The SMN2, highly homologous gene of SMN1, is a well-established disease-modifying gene for SMA and has been shown to decrease the severity of type I-III SMA in gene dosage analyses (11, 15, 19). The copy number of SMN2 also correlates with longer survival of individuals affected with type I SMA (15). Thus, the quantitative analysis of SMN2 gene enables it possible to predict that an infant with homozygous deletion of SMN1 develop type I, II or III SMA. Although we did not carry out the assay of SMN2 gene in the present study, our real-time quantitative PCR analysis could produce sufficient results.
In conclusion, we detected SMN1 deletion carriers in a general population and calculated the prevalence as the advantages of real-time PCR with SYBR Green I. With relatively high frequency of SMA compared with other autosomal recessive disorders, the carrier detection method using real-time PCR could be a useful tool for genetic counseling.



 XML Download
XML Download