

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cervical pregnancy is a serious complication of pregnancy with a rare incidence of one per 2,400 (1) to 18,000 pregnancies (2). The diagnosis is based upon a high degree of suspicion and confirmed with either vaginal or abdominal sonography (3, 4). In the past, hysterectomy was often the only choice available because of profuse hemorrhage that accompanied the attempts of removal of the cervical pregnancy. With the development of high resolution ultrasound and sensitive serum β-human chorionic gonadotrophin (β-hCG) assay, cervical pregnancy is diagnosed much earlier. Therefore, various conservative surgical techniques are performed in an effort to avoid hysterectomy and preserve fertility. The surgical techniques include intra-cervical balloon tamponade after cervical curettage (5), cervical cerclage (6, 7), angio-embolization of feeding uterine arteries (8, 9), curettage and local prostaglandin injection (10), hysteroscopic resection (11, 12) and bilateral ligation of uterine or hypogastric arteries (13, 14). Nevertheless, such surgical methods still carry the risk of uncontrollable bleeding and non-surgical methods using methotrexate (MTX) (15-17), actinomycin-D (18) and etoposide (19) have recently been developed. Surgical techniques are generally applied only when chemotherapy fails or in emergency conditions of life-threatening acute hemorrhage (20).
In this study, we describe the clinical course of a series of patients treated for cervical pregnancy with or without MTX. The effects of MTX treatment is also evaluated.
MATERIALS AND METHODS
During the 85-month period from January 1993 through February 2000, a total of 52,555 deliveries were performed at the Department of Obstetrics & Gynecology, Samsung Cheil Hospital & Women's Healthcare Center, Sungkyunkwan University, School of Medicine, Seoul, Korea. Thirty-one cervical pregnancies were detected during the same period. A retrospective study was conducted to describe the clinical course of a series of patients treated for cervical pregnancy with or without MTX. Of these 31 cases, 22 patients were treated with MTX chemotherapy and the remaining nine patients were treated with surgical procedures without MTX treatment. Clinical characteristics, surgical procedures, MTX regimens used, concomitant procedures, treatment results and complications were retrospectively reviewed with medical records.
Cervical pregnancy was diagnosed by ultrasound (21). The diagnostic criteria included are as follows; first, there is no evidence of an intrauterine pregnancy. Second, the cervix is distended and the uterus is hourglass shaped. Third, there is conceptal or placental tissue in the cervix. Fourth, internal os of the cervix is closed. The gestational age was determined by the size of gestational sac by ultrasound (22).
The MTX regimens varied among the physicians. It was given systemically in a high-dose regimen (a dosage of 100 mg/m2 plus a dosage of 200 mg/m2 in normal saline solution 500 mL, intravenous injection) with folinic acid rescue, given in low-dose prolonged regimen (1.0 mg/kg for a single dose given every other day for 4 doses, intramuscular injection) (23) or given as a single 50 mg MTX regimen (24). Folinic acid rescue (0.1 mg/kg) was used after systemic MTX administration. Repeat treatments were indicated when the decrease in serum β-hCG was below 15%, if vaginal bleeding persisted or if gestational mass enlarged.
Patients were monitored with ultrasound and serum β-hCG level once a week until resolution of β-hCG level. After serum β-hCG level normalization, the patients were followed up with ultrasound once a month until the cervical mass resolved.
Student's t-test and Fisher's exact test were used for statistical analysis. A p value of <.05 was considered statistically significant.
RESULTS
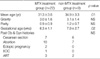
The incidence of the cervical pregnancy was one in 1,695 live births. Patient characteristics of the MTX and non-MTX treatment groups are compared in Table 1. The mean age of the MTX treatment group was 31.3±3.6 yr, and 34.9±3.3 yr in the non-MTX treatment group. The mean gravidity and parity were not statistically significant. The mean gestational age was 6.3±1.1 and 7.9±2.7 weeks in the MTX and the non-MTX treatment groups respectively. There were significant differences in patient age and gestational age. Past histories of the patients were as follows; 25 had elective or spontaneous abortions, 13 had Cesarean deliveries, two had tubal pregnancies, one had cone biopsy and resultant incompetent internal os of the cervix and five developed cervical pregnancy during in vitro fertilization (IVF) with embryo transfer (ET).
The clinical presentations and treatment outcomes in the non-MTX treatment group are summarized in Table 2. The mean gestational age was 7.9±2.7 weeks (range 6-13) and regular heartbeat was detected in three cases (33%). Dilatation and curettage (D&C) was performed in all nine cases. However, three patients underwent total hysterectomy due to uncontrollable uterine bleeding during D&C and five patients required adjuvant procedures (gauze packing into the cervical canal, local vasopressin injection and compression with ring forceps, recurettage, Foley catheter ballon tamponade, or ligation of the descending branches of uterine arteries) to control the bleeding from the cervical canal. Five patients received blood transfusions.
The clinical presentations, MTX regimens used and treatment outcomes in the MTX treatment group are summarized in Table 3. The mean gestational age was 6.3±1.1 weeks (range 5.3-9.6) and regular heartbeat was detected in 11 cases (50%). Twelve patients received a systemic high dose MTX regimen, four received a systemic low dose MTX regimen and one received a single dose MTX regimen. Four patients received a combination of a systemic high dose MTX regimen with trans-cervical intra-amniotic injections of 2 mEq KCl or 2 mL MTX and one received a single-dose MTX regimen with trans-cervical intra-amniotic injection of 2 mEq KCl. A single course of systemic MTX treatment failed to cease the cardiac activity in all four cases beyond 7 weeks of gestational age. The mean number of MTX treatment courses was 2.5±1.8 (range 1-7). The mean initial β-hCG level was 44,183 mIU/mL (range 556-331,000). The mean time until β-hCG level resolution after treatment initiation was 60.3±32.5 days (range 14-140). A gradual decline in β-hCG level after MTX treatment initiation was noted in all cases but for one in which β-hCG level rose progressively until 7 days after the fetal demise. After MTX administration, 19 patients underwent sonographic follow-up and 13 had a disproportionately enlarged cervical mass despite β-hCG level declination. The mean period from treatment initiation until sonographic non-visualization of the cervical mass was 72.4±43.8 days (range 12-180). MTX-related side effects such as nausea, vomiting, elevated serum liver enzyme activities and fever developed in four patients (18%) after systemic injection. All of the reported side effects were self-limited and subsided within 14 days. Seven patients received blood transfusions. During the follow-up period, fourteen patients (63.6%) did not require any concomitant procedures whereas the other eight (36.4%) underwent various concomitant procedures. Concomitant surgical procedures (simple curettage, curettage and Foley catheter tamponade, cervical cerclage, ligation of the descending branches of uterine arteries, or ligation of the hypogastric arteries) in conjunction with MTX therapy were performed in cases of uncontrollable bleeding requiring transfusion. In all cases, the uterus was preserved and menstrual patterns returned to normal. After treatment, fifteen women attempted subsequent pregnancies and three delivered normal and healthy babies.
Regular heartbeat and gestational age were considered important factors requiring concomitant procedures in the MTX treatment group. However, these factors failed to show statistical significance after separate analysis (Table 4, 5).
There were two cases of heterotopic cervical pregnancy after IVF with ET. One case is a single cervical pregnancy and a single intrauterine gestation (Table 3, Case 8) and another is a single cervical pregnancy and triple intrauterine gestation (Table 3, Case 9). Elective abortions were performed on all fetuses in the cervix and uterus with transvaginal ultrasound-guided intra-amniotic MTX injection. All gestational tissue within the uterus and cervix was absorbed spontaneously without the need of curettage.
There were two interesting cases in the MTX-treatment group. One patient (Table 3, Case 1) had profuse uterine bleeding requiring transfusions 37 days after the first MTX chemotherapy. Laparotomy for uterine artery ligation was attempted but failed due to a large irremovable cervical mass reaching the pelvic bone. Instead, a second course of systemic high dose MTX was administered and uterine bleeding ceased 2 days afterwards. The cervical mass completely resolved 180 days after beginning of the first MTX treatment.
Another patient (Table 3, Case 10) of gestational age 9.6 weeks presented with a 2 cm dilated exocervix with bulging amniotic sac. Local injection of MTX agent could not be given in fear of membrane rupture and bleeding. Systemic high dose MTX therapy was initiated but fetal cardiac activity failed to cease even 7 days after MTX injection. On day 10, MTX 50 mg was locally instilled into the amniotic cavity under transabdominal sonographic guidance. However, the fetal cardiac activity persisted. After the fourth MTX administration, anhydramnios and upward fetal growth resulted in exocervix closure and intra-fetal injection of 2 mEq KCl was possible. This method proved to be effective in halting the fetal cardiac activity. After 2 months, the dead fetus spontaneously passed but the placenta was retained in the cervix. Curettage was performed to remove the retained placenta but bleeding of about 1,000 mL occurred within 20 min. The bleeding was managed with bilateral hypogastric artery ligation and Foley catheter balloon tamponade in the cervical canal. Uterine bleeding continued at a rate of 20 mL/hr for 24 hr then gradually decreased and eventually stopped 2 days after the surgery.
DISCUSSION
Cervical pregnancy is a rare form of ectopic gestation which is often associated with a significant morbidity and a disastrous effect on future fertility. The true incidence of cervical pregnancy cannot be precisely determined, but reviews of literature indicate that the incidence may be on the rise from one in 2,400 (2) to 18,000 pregnancies (1). In our study, the incidence of the cervical pregnancy was one in 1,695 live births. The incidence also appears to be increasing, in part, due to recent developments in novel forms of assisted reproductive techniques, especially IVF and ET (25). Improper placement of the fertilized ovum and manipulation within the cervical canal could increase the likelihood for cervical implantation (26). Cervical pregnancy developed in 5 patients during IVF and ET in our study. Thirteen of our patients had a history of Cesarean delivery and twenty-five patients had elective or spontaneous abortion.
The success rate of MTX treatment in cervical pregnancy has been reported as high as 81.3% (27). MTX chemotherapy combined with adjuvant conservative procedures has a success rate of 94% and 91% in the viable and the non-viable cervical pregnancy groups respectively. Fetal viability may not affect treatment efficacy. The viable and non-viable group each requires concomitant minor operative procedures during the treatment course in 43% and 13%, such as endocervical curettage, cervical balloon tamponade, and uterine artery embolization (28, 29). An average of 53 days is required after initiation of MTX therapy for the uterus to return to nonpregnant status (28). In our study, the mean period from treatment initiation till sonographic resolution of the cervical mass was 72.4 days. The viability of the cervical pregnancy and the size of gestational sac may not affect the efficacy of treatment. However, the concomitant procedures were required 54% in the viable and 18.2% in the non-viable group, and 50% in the beyond 6 weeks of gestational age and 20% in the less than 6 weeks of gestational age group, respectively. Therefore, physicians must consider the need of concomitant procedures in cases with fetal heart beat or beyond 6 weeks of gestational age. With MTX chemotherapy and concomitant use of surgical procedures in selected cases, the uterus could be preserved in all cases (100%), this result concurs with the study of Kung et al. (28).
The regression of the cervical hypervascular mass after MTX treatment is related to the decline in the β-hCG level. Although a disproportionately enlarged cervix will progressively shrink as β-hCG level declines, enlargement may still be present even after serum β-hCG level becomes undetectable (30). We observed 13 cases of disproportionately enlarged cervical mass despite β-hCG level decline. Nevertheless, no attempt should be made to reduce the size of the asymptomatic hypervascular cervical mass as such manipulation of the cervix may cause bleeding fraught with serious consequences.
MTX-related side effects such as gastrointestinal upset, pharyngitis, stomatitis, elevated serum liver enzyme activities, leukopenia, thrombocytopenia, conjunctivitis, and fever developed in 14 (29%) of 48 patients after the systemic injection (28). In our study, MTX-related side effects was noted in 4 (18%) out of 22 patients.
Based on our study, systemic MTX administration combined with intra-cardiac feticide with either MTX or KCl appears to be effective treatment in cases of viable cervical pregnancy beyond 7 weeks of gestational age. Systemic MTX administration alone was effective in almost all cases of nonviable and viable cervical pregnancy at gestational age below 7 weeks. However, if the bleeding is not profuse after one or two courses of MTX, the patient may be observed until the cervical mass resolves. With profuse or prolonged bleeding, blood transfusions may be required and concomitant procedures for bleeding control should be considered.
In conclusion, early diagnosis, appropriate MTX regimen and combination of necessary adjuvant conservative procedures could contribute to successful treatment with preservation of the uterus and future reproductive ability.




 XML Download
XML Download