

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thymic carcinomas are unusual malignant neoplasms that have wide variety of morphologic appearances. Mucoepidermoid carcinomas of the thymus are extremely rare malignant mediastinal neoplasms and account for 2% of thymic carcinomas (1, 2). Until now, radiologic reports of mucoepidermoid carcinoma of the thymus have been rare, but the described gross findings are multilocular cystic structures with focal areas of induration within the walls of the cyst or well-circumscribed homogeneous tumor masses (3). We report a case of mucoepidermoid carcinoma of the thymus with radiologic and histologic findings.
CASE REPORT
A 53-yr-old male was admitted to our hospital complaining of right chest pain. The physical examination and laboratory studies were unremarkable.
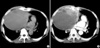
Erect posteroanterior and lateral radiographs of the chest showed a well marginated anterior mediastinal mass in the entire right lung zone, compressing the lower trachea, right bronchus, and heart toward the left side (Fig. 1). CT scan of the chest demonstrated a 20×16×10 cm-sized, cystic mass with focal heterogeneously enhanced solid portion anteromedially in the anterior mediastinum. Direct invasion of the anterior chest wall and pericardium by the mass was suggested, because pericardial fat plane was obliterated and the margin between the mass and the adjacent right anterior chest wall and pericardium was indistinct (Fig. 2). Minimal amount of right pleural effusion and pericardial effusion were associated.
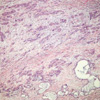
At surgery, after aspiration of fluid within the cystic mass, pericardial invasion was noted. Thus, partial resection of the mass was done. Histologically, squamoid tumor cells formed cords or solid sheets within the fibrous stroma admixed with mucin-secreting epithelium lining gland-like spaces (Fig. 3). The final pathologic diagnosis was poorly differentiated mucoepidermoid carcinoma of the thymus. The patient died in one year after surgery despite postoperative radiation therapy.
DISCUSSION
The thymic carcinomas are a heterogeneous group of aggressive epithelial malignancies that have a strong propensity for early local invasion and wide spread metastases. Squamous cell carcinoma and lymphoepithelioma-like carcinoma are the most common cell types and usually occur in middle-aged men with a mean age of 46 yr (4-6). Radiologically, thymic carcinomas commonly manifest as large, poorly defined, infiltrative anterior mediastinal masses and associated with areas of necrosis, hemorrhage, calcification, or cyst formation (2, 6, 7).
Mucoepidermoid carcinoma was first recognized as a distinct pathologic entity in salivary glands by Stewart et al. in 1945. Since then, this tumor has been identified in several other organs, including lung, esophagus, anus, cervix, and skin. Although extremely rare, mucoepidermoid carcinomas of the thymus have also been described (3). So far, only thirteen cases have been reported in the English literature (3, 8, 9). The patients ranged in age from 17 to 66 yr, with a mean age of 35 yr on reported cases (3). Clinically, most patients were asymptomatic or had symptoms of chest discomfort, retrosternal pain and dyspnea.
Radiologic reports of mucoepidermoid carcinoma of the thymus were rare. But two distinct gross findings, as described by Moran et al., are multilocular cystic structures varying in size with focal areas of induration within the walls of the cyst and well-circumscribed, homogeneous tumor masses (3). Our case presented as a 20 cm-sized, cystic mass with focal heterogeneously enhanced solid portion anteromedially in the anterior mediastinum. The invasion of anterior chest wall and pericardium was suspected due to indistinct margin between the mass and adjacent right anterior chest wall and pericardium, and surgically proved.
Histologically, the lesions showed a spectrum of features that ranged from those of well-differentiated, to moderately well-differentiated, to poorly differentiated mucoepidermoid carcinoma, with sheets and solid islands of squamoid cells admixed with mucin-secreting epithelium lining gland-like spaces (3). The histogenesis of these tumors is still unclear; however, the demonstration of transitions between the tumor cells and the epithelium lining the cysts as well as residual non-neoplastic thymic remnants within the walls of the cysts in four of six cases supports the theory that these tumors arise from thymic epithelium (3).
Differential diagnoses of masses of the anterior mediastinum associated with extensive cystic changes include thymic cysts, thymomas, teratomas, seminomas, Hodgkin's disease, and metastasis (10-14). And also mucoepidermoid carcinoma of the thymus should be included in the differential diagnosis, although the carcinoma is an exceedingly rare anterior mediastinal malignant tumor (3). It is very difficult to differentiate from each other by only radiologic findings (10-14). However, mucoepidermoid carcinoma of the thymus should be considered when a large cystic mass with focal induration within the anterior mediastinum on CT scan is noted.

 XML Download
XML Download