

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bronchial atresia resulting from a localized defect in normal bronchopulmonary embryogenesis is a rare disease. It can produce emphysematous changes in the affected pulmonary segment or lobe with or without dyspnea and/or episodic pulmonary infection. However, bronchial atresia predisposed to recurrent pneumothorax is a very rare clinical presentation. We herein report a case of bronchial atresia associated with pneumothorax which was successfully treated with lobectomy.
CASE REPORT
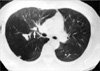
A 32-yr-old Korean male patient was admitted to Inha University Hospital, Incheon, Korea due to dyspnea and right chest pain for 1 day. On physical examination, the breath sound in the right lung fields was decreased without shifting of the maximal point of the cardiac impulse. He had a history of the right pneumothorax one and a half years ago, which was treated with tube thoracostomy. He had no history of pulmonary or bronchial tuberculosis before this admission. He was a smoker. The posteroanterior chest radiograph revealed increased radiolucency along with overinflated lung parenchyma and sparse vasculature in the upper half of the right lung. Also note v-shaped branching opacity was in the right parahilar area. Pneumothorax was associated in the right lower pleural cavity (Fig. 1). A 32 Fr chest tube was inserted into the right pleural cavity. The chest CT taken in the state of full expansion of the right lung after tube thoracostomy showed a branching soft tissue density in the region of the posterior segment of the right upper lobe. The orifice of the posterior segmental bronchus was visualized but the orifice of the subsegmental branch of the posterior segmental bronchus could not be visualized separate from the origin (Fig. 2). There were no endobronchial lesions in the bronchial tree on the bronchoscope and each orifice of the segmental bronchi of the right lung was seen normal. His forced expiratory volume at 1-sec (FEV1) was 3.49 L (91%) and forced vital capacity (FVC) was 4.57 L (100%). Perfusion lung scan showed a perfusion defect in the right upper lobe. Exploratory thoracotomy was done via muscle sparing vertical thoracotomy skin incision. There was a localized emphysematous change in the posterior segmental area of the right upper lobe with the apical pleural adhesion and the remaining lungs were normal. Right upper lobectomy was successfully undertaken. The pathological findings of the resected right upper lobe showed overinflation of the posterior segment. There were no obstructed lesions of the orifices of the three segmental bronchi of the right upper lobe. However, one of the subsegmental branch of the posterior segmental bronchus was obstructed and there was a 2.5×1.5×1.5 cm sized cystic mass containing brownish mucus material at the distal portion of the obstructed subsegmental bronchus. The cystic mass was not connected with other bronchial trees. Microscopically the distal air spaces of the atretic segmental bronchus showed overinflation only. However the foci of the subpleural bullae in the overinflated segment were observed (Fig. 3). His postoperative course was uneventful. He was discharged on the post-operative 7th day. He has been well 1.6 yr after the operation.
DISCUSSION
Bronchial atresia is a rare disease, which develops due to the failure of embryogenesis of the segmental or lobar bronchial tree. Since the first report of bronchial atresia by Ramsay et al. in 1953, there have been many illustrations and reports about bronchial atresia (1-8). According to the reports, most of the patients with bronchial atresia were asymptomatic and it was diagnosed incidentally in the second or third decade of life on routine chest radiography (2-4). The common radiographic findings of bronchial atresia are hyperinflation of the involved lung parenchyma and collapse of the affected lobe with a radioopaque extrahilar mass with mucocele in patients who had pulmonary symptoms such as fever, cough, and shortness of breath due to recurrent pulmonary infection or overinflation of the involved lung parenchyme (3, 4, 6, 8). However, bronchial atresia associated with pneumothorax is extremely rare in spite of overinflation of the involved lung parenchyma. Such a case was only reported by Berkman et al. (5) according to the clinical findings. Here we report a case of bronchial atresia in the subsegmental branch of the posterior segmental bronchus of the right upper lobe associated with mucocele and recurrent spontaneous pneumothorax, which was treated with right upper lobectomy. The resected specimen showed atresia of the subsegmental branch of the posterior segmental bronchus of the right upper lobe with hyperinflated lung with subpleural bullae. So the bronchoscopic finding showed normal orifice of the each bronchus. The cause of pneumothorax was thought to be due to the rupture of the bulla in the hyperinflated lung segment. The exact mechanism of bulla formation of the affected lung parenchyma could not be proved. However, we think the bullous change have been resulted from mechanical stress to the alveoli wall from hyperinflation of the lung parenchyma distal to the atretic bronchus due to aeration by check-valve mechnanism through the collateral channels of the interalveolar pores of Kohn and bronchoalveolar channels of Lambert.


 XML Download
XML Download